The computed tomography method is often used to diagnose respiratory pathologies. This is a safe X-ray examination that takes 15-30 minutes and allows you to assess the condition of the lungs. The images are formed from 1000 layer-by-layer images of tissues. Any deviations from the norm are visible on them. Based on the images, the doctor can accurately diagnose and prescribe effective treatment. The method is used to clarify pneumonia, tuberculosis, chronic diseases, neoplasms, and assess lung function.
What is CT?
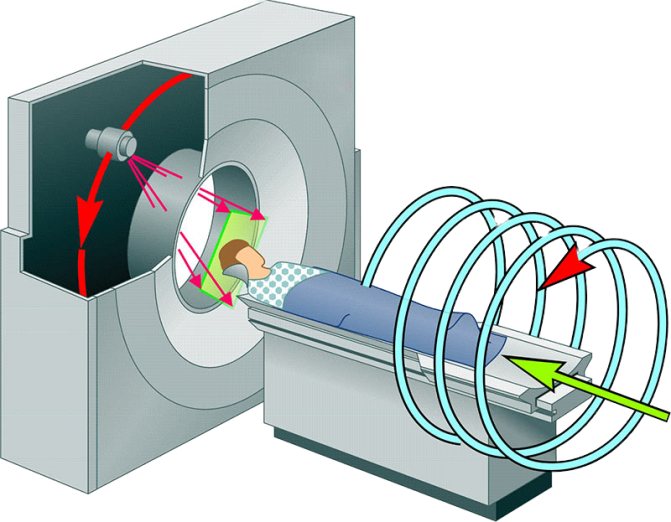
A CT scanner is a scanner with X-ray sensors. The radiation dose is safe for the body. The scanner contains a table on which a person sits. During the study, the patient lies still and follows the doctor's instructions. Over the course of half an hour, the scanner rotates around the table and takes a series of pictures.
The tomograph has precise settings for layer-by-layer scanning of tissues. If necessary, the device takes pictures every 0.5-1 mm. With this resolution, it is impossible to miss even minimal changes in tissues.
At the end of the study, computer equipment creates a digital 3D model of the respiratory system from a series of images. The attending physician can examine the lungs in any projection and examine problem areas as closely as possible.
After CT scan of the lungs
Immediately after the examination in our center, the patient receives a recording of the study (lung scans) on a high-resolution DVD and a commentary from a radiologist. No rehabilitation is required—immediately after a CT scan of the lungs, you can return to your usual activities. If a CT scan of the lungs with contrast (angiography) was performed, then after diagnosis you should drink more clean water than usual so that the iodine-containing drug is eliminated from the body faster.
The doctor will carefully examine scans of the lungs in three projections. A CT scan will show focal changes in the lungs with pneumonia, tuberculosis, as well as neoplasms, damaged vessels and other abnormalities, if any. Then the doctor will write a conclusion and send it to the patient by email.

What diseases are diagnosed by this method?
A pulmonologist, surgeon, oncologist or internist can refer you for a CT scan of the lungs. The list of diagnoses is extensive:
- pneumonia;
- tuberculosis;
- chronic obstructive pulmonary disease;
- damage to the lymphatic system;
- benign and malignant neoplasms;
- metastases in the lungs;
- parasitic, fungal infections;
- sarcoidosis;
- silicosis;
- anthracosis;
- pulmonary embolism;
- traumatic damage to the respiratory system;
- fluid in the pleural cavities;
- fibrosis of lung tissue;
- interstitial lung diseases (fibrosing alveolitis, vasculitis).
Advantages of the method:
- maximum information content;
- 3D image of tissues;
- you can accurately determine the location, size, nature of the pathological focus;
- high detail of images;
- safety for the body (low dose of radiation);
- assessment of all lung segments without blind spots;
- detection of tumors up to 5 mm in size at the initial stages.
Focal changes in the lungs on CT
Since the thickness of the tested layer on CT is 1-2 mm, focal formations in the lungs , characteristic of many serious diseases, are clearly visible in the images obtained during the examination.
The norm on a CT scan of the lungs describes the following structures of the chest and their parameters:
- lung fields and chest contours;
- condition of the pleura and absence of accumulations (purulent secretion/ fluid );
- location of the mediastinum – without expansion or displacement;
- absence of neoplasms in the mediastinum;
- increased size of the mediastinal lymph nodes – not recorded;
- the lobes and segments of the lungs are not differentiated, there are no fresh or old single foci of compaction.
Focal formations are characteristic of tuberculosis, tumor diseases, and complicated types of pneumonia. Primary diagnosis using X-ray or fluorography reveals lesions larger than 10 mm; the efficiency of recognizing single lumps is no more than 1%. That is why dynamic CT (with the addition of a contrast agent) is the most effective way to early diagnose respiratory pathology.
Types of focal formations
Pulmonary lesions are classified by size, location, density and number (prevalence). Lung compactions on computed tomography vary from 1-2 to 10-15 mm; their location can be the interstitium (lung tissue), pleura, walls of the bronchi and blood vessels.
Lung screening shows that up to 80% of focal formations are benign, especially with diffuse distribution of nodules. Lesions appear as a result of exposure to the following factors:
- calcifications – due to past inflammatory diseases;
- fibrosis of any etiology (overgrowth of connective tissue);
- fungal infection of the lungs (candidiasis, blastomycosis, cryptococcosis, etc.);
- hematomas and lung contusion ;
- airway obstruction – pulmonary atelectasis
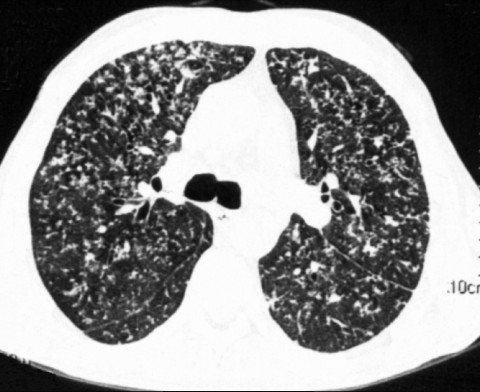
On CT images, focal changes may appear as rounded/blurred shadows or lightened areas. Thus, one of the complications of chronic bronchitis may be an increase in air-containing bubbles. When performing a CT scan, pulmonary emphysema is visualized as a violation of the pulmonary pattern and the spread of “transparency” zones. Healthy lung tissue has a dense structure with clearly defined edges, while areas with emphysema are characterized by increased airiness.
Computed tomography examination is indispensable for complications of the bronchopulmonary system caused by the patient’s acute condition - intoxication, renal failure, myocardial infarction. CT scan reveals pulmonary edema , which can be fatal if not diagnosed promptly.
Metastases in the lungs on CT scan with contrast
The effectiveness of detecting metastases in the lungs during CT screening reaches 55-60%. Enhancement with a contrast agent is carried out to obtain clearer images, which can be used to determine the location of metastases and the extent of their growth into neighboring organs.
The lungs can act as a site of concentration of metastases for malignant neoplasms of other organs, since cancer cells easily enter the mediastinum area through the lymphatic vessels. A CT scan with contrast recognizes metastases whose diameter does not exceed 0.5 cm. In this case, single metastatic foci do not carry any symptoms and can only be detected with a control CT scan during treatment of lung cancer. Multiple focal lesions with metastases are accompanied by deterioration of health and increased cough and shortness of breath.
CT scan for pulmonary tuberculosis
Diagnosis of pulmonary tuberculosis is made based on computed tomography data and patient test results (sputum, saliva, bronchoscopy). The initial definition of the disease is characterized by subpleural foci in the lungs on CT images infiltrates and compactions located under the pleura.
Focal lesions in tuberculosis have a “frosted glass” appearance and are accompanied by enlarged lymph nodes. If such changes are present during an X-ray examination using a CT scan of the lungs, pneumonia is differentiated from primary tuberculosis. The scan detects compactions, contamination or areas of decay in the lungs with a diameter of 1 mm, which makes it possible for early recognition of the disease.
CT images give an idea of the form of diagnosed tuberculosis (focal, disseminated, cavernous, cirrhotic) and the pathological changes present in the lung tissues.
Computed tomography for tuberculosis, as for lung cancer, is actively used not only to make an accurate diagnosis, but also to monitor the patient’s condition during treatment.
When does the doctor refer for a CT scan?
Symptoms indicating diseases of the respiratory system are shortness of breath, prolonged dry or wet cough, which is accompanied by fever. Today, computed tomography is widely used to detect lung lesions due to coronavirus infection.
Often the reason for undergoing an examination is pain in the chest, which is accompanied by cold sweat, pallor or cyanosis of the skin. Such symptoms are a consequence of arterial pulmonary thromboembolism.
Other diseases can also cause damage to the respiratory system: cirrhosis, hepatitis, HIV, sarcoidosis. Tomography will allow the doctor to get a complete picture of the disease.
Benefits of Lung CT
- Diagnosis is quick and without discomfort. In certain cases, CT acts as an alternative to instrumental-invasive methods of examining the respiratory tract - bronchoscopy or pulmonary endoscopy.
- CT scans are highly informative compared to X-rays or fluorography. CT scan of the lungs is better than MRI in showing pneumonia, tuberculosis, and mediastinal tumors. With the help of computed tomography, respiratory tract organs, bones and blood vessels can be examined in different planes, and even initially determine the type of neoplasm detected (from 5 mm).
- Diagnostics is not contraindicated in patients with implants in the mediastinum and does not cause panic in claustrophobia.
- A CT scan of the lungs without contrast does not require special preparation - the examination can be completed immediately on the day of your visit.
- CT is suitable for annual preventive screening of lung cancer, as well as for monitoring the recovery of the airways after pneumonia, tuberculosis and other diseases.
- You don’t have to do X-rays and fluorography - a CT scan of the lungs will show everything that is necessary. The study is recorded in high definition on DVD, which meets the requirements of attending physicians and preparation for precision surgical operations.
Who is the procedure contraindicated for?
- Restrictions apply to patients weighing more than 145 kg. Many devices are simply not designed to carry such a large weight.
- CT scanning is not recommended for pregnant women.
- The study cannot be carried out if the patient has severe diseases of the nervous system.
- CT angiopulmonography is not performed for people with renal failure, severe diabetes mellitus, thyroid pathologies and an allergy to iodine, which is contained in the X-ray contrast agent.
CT lungs with contrast
In some cases, the patient is advised to undergo a CT scan of the lungs with contrast. Contrast is a special iodine-containing drug that is administered intravenously to the patient before diagnosis. CT scan of the lungs with contrast allows you to visualize blood vessels and differentiate neoplasms.
The contrast agent passes through the circulatory system, “staining” the vessels and organs from the inside. The iodine molecules included in the contrast allow the drug to absorb x-rays more actively and make soft tissues brighter on tomograms. A chest CT scan with contrast is done to assess the condition of the pulmonary vessels, blood circulation, and also to increase the information content of the examination when necessary, for example, when diagnosing a neoplasm.
Typically, a contrast study is prescribed by a doctor. Sometimes such a need arises after the first scan without contrast, if the patient has detected signs of suspicious pathological processes that need to be excluded or examined in more detail. A single repeat scan is absolutely safe for the patient. It is also possible to initially distinguish a benign neoplasm from an oncogenic process using a CT scan of the lungs with contrast.
For fast, precise and painless administration of the drug, we use an injector device. The examination with contrast takes about 15-20 minutes.
The drug for contrast enhancement of CT scans does not harm the body and is eliminated from the body within 24 hours after a CT scan of the lungs. To assess the condition of the chest and lung organs, for example, to clarify the degree of their damage during pneumonia, detect tuberculosis, bronchitis, etc., native computed tomography without contrast is sufficient.
How is a computed tomography scan of the lungs performed?
The patient is positioned on the tomograph table with his hands behind his head. The machine begins to rotate, taking a series of X-ray images. Many patients fear that they will feel uncomfortable in a confined space. But there is no need to worry about this - in modern tomographs there is no closed space.
The doctor operating the machine may ask the patient to hold his breath for 10-15 seconds. An important condition is that you need to lie still while the tomograph is operating, otherwise the images will be blurry.
In what cases is a CT scan of the lungs prescribed?
For CT scans of the lungs, the indications are as follows: prolonged cough, including with atypical contents, blood, elevated body temperature, general weakness, headaches and chest pain, previous chest injuries, suspicion of the presence of foreign bodies in the lungs, cyanosis of the lips and etc.
Lung tomography is prescribed to assess the extent of surgical intervention, when assessing the effectiveness of radiation and chemotherapy, and also in cases where alternative methods do not reliably and unambiguously identify the pathological focus.
Where can I get a CT scan?
Sign up for a computed tomography scan at the MRI Center by phone or through the feedback form on the website. Doctors of the highest category, polite staff, and the latest generation tomographs - Philips, Siemens, Toshiba - are waiting for you. You will receive high-quality images, an expert opinion and a chance for a speedy recovery.
There are no queues at our diagnostic centers - studies are carried out by appointment for a specific time. The air in the rooms is disinfected after each patient, all surfaces are thoroughly treated with antiseptic solutions.
CT scan of the chest - what the diagnosis shows
Primary diagnosis using radiography usually reveals large lesions ranging in size from 1 cm, while the sensitivity of X-rays for recognizing single lumps is very low. CT plays a special role in the early diagnosis of respiratory disorders - by obtaining a series of thin layer-by-layer images of the chest, doctors can assess the general condition of the structures in this area, verify the smallest inflammatory, infectious, oncological and other processes.
A CT scan of the chest cavity shows the presence of the following pathologies:
- focal formations in the lungs, bronchi;
- enlarged mediastinal lymph nodes, their sizes;
- fungal infections;
- acute and chronic bronchitis;
- lymphoma and other disorders of the lymphatic system;
- fibrosis;
- calcifications;
- presence of free fluid in the chest;
- lung contusion, hematoma, other consequences of traumatic injury;
- acute and chronic forms of pneumonia, tuberculosis;
- obstructive pulmonary diseases;
- emphysema;
- atelectasis;
- pulmonary edema, CT shows the localization of edema, severity, etc.;
- bronchiectasis;
- malignant and benign space-occupying formations of the lungs, bronchi and other structures;
- hamartoma, other congenital anomalies of organ development;
- inflammation of the pleura;
- thromboembolism of pulmonary and great vessels;
- inflammation leading to damage to lung tissue and capillaries;
- systemic lung diseases.
Computed tomography of the lungs detects the smallest nodules, which are characteristic of the initial stage of lung cancer.
Chest CT without contrast is often used in clinical examinations as a screening method.
CT scans of the heart, bronchi, and CT scans of the lungs are normally characterized by the presence in the images of organs and tissues of normal density, homogeneous structure, without the presence of foreign bodies, focal changes, without vasodilatation, infiltrates and free fluid in the cavity. In this case, the pulmonary fields, roots, bronchi, trachea, heart structures are not changed, the mediastinal lymph nodes are not enlarged, bone-traumatic disorders are not detected, the great vessels are unchanged, and the heart is of normal configuration.
Lung cancer on CT photo
Can a CT scan be used to diagnose lung cancer? Computed tomography for malignant tumors of the lung is the main informative type of diagnosis after obtaining primary information using chest radiography.
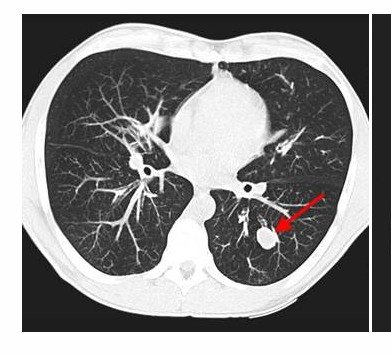
The main signs of the presence of malignant focal changes in the lungs on CT are blurred or radiant contours of the formation, infiltrative growth, unevenness of the structure, and sometimes on tomograms the merging of foci with each other is visualized.
In case of peripheral lung cancer, the conclusion may contain information about the disintegration of the node and the active nature of the growth of the pathology.
Adenocarcinoma appears as a round or irregular nodule on imaging, with a maximum thickness of less than 3 cm. Invasive adenocarcinomas may have a variable appearance, ranging from consolidation to multifocal nodules.
Squamous cell carcinoma, when centrally located on CT images, is characterized by intraluminal obstruction, which causes obstructive pneumonitis or lung collapse. If the formation is located on the periphery, a solid nodule with or without a clear border is visualized. Characterized by infiltrative growth, cavitation is common.
The small cell form of lung cancer is most often located centrally, growing from the lobar bronchi. On images it is therefore visualized as an intrathoracic disorder, which is accompanied by widening of the mediastinum. The mediastinal lymph nodes are often involved in the process. This form of cancer is a common cause of obstruction, thrombosis or direct infiltration.
Rarely, bronchioloalveolar cancer is a type of adenocarcinoma. In most cases, such a formation is peripheral; on photographs it appears as a diffuse decrease in the density of the lung parenchyma, like ground glass.
A CT scan of the mediastinum shows the involvement of other structures of the thoracic region and lymph nodes in the tumor process, and to assess the spread of the disease, the radiologist makes fine frontal and sagittal reformatting to visualize the pulmonary roots and the affected part of the chest.
CT diagnosis of lung cancer also verifies tumor growth into the lumen of the bronchus, which causes narrowing of the latter. In the photographs, the tumor node itself is visualized as white in color in the lumen of the bronchus. You can also notice an increase in the density of the corresponding lobe or segment that is ventilated by this bronchus.
MSCT of the lungs is also done to assess the spread of tumor cells to the lymph nodes. For example, with lymphangitis, you can notice the appearance of specific “paths to the root” in the photographs.
The lungs can act not only as the site of primary tumors, but also as the location of metastases for cancer of the stomach, testicle, esophagus and other organs, since cancer cells easily penetrate into the mediastinum through the lymphatic system. Thanks to CT with contrast, it is possible to recognize secondary tumors whose size does not exceed a fraction of a centimeter.
Note that to diagnose primary tumors and metastases in the lungs, CT with contrast is performed; thanks to this enhancement, the exact sizes of the foci, their blood supply and connection with adjacent organs and tissues are assessed, it is possible to accurately verify not only single foci of the tumor process, but also numerous volumetric formations of minimal sizes.
Will a CT scan show sarcoidosis?
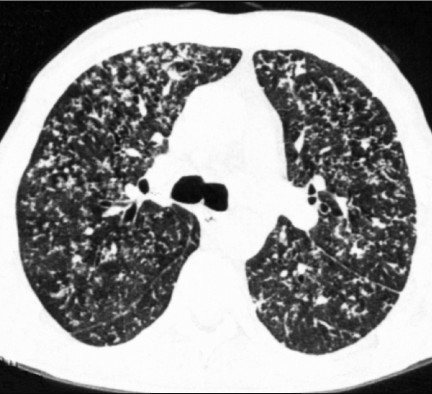
The main signs of this disorder are areas of compaction in the lungs on computed tomography, symmetrical bilateral tissue compaction in the form of multiple small foci of the lungs on CT images, which are located along the vessels, pleural layers, bronchi of the perilymphatic type. Also, sarcoidosis is characterized by pleural effusion in the active stage of the disease; in advanced forms, fibrous changes, traction bronchiectasis, etc. are visualized in the images.
Areas of compaction in sarcoidosis are characterized by a ground glass type, the nodes often have calcifications along the periphery. Each node is usually quite distinct, which distinguishes sarcoidosis from neoplastic lymphadenopathies.
What does pulmonary emphysema look like on CT images?
The main signs of the disease include the presence on tomograms of a rarefaction of the pulmonary pattern, dilatation of the branches of the pulmonary arteries, which abruptly break off along the periphery, flattening of the domes of the diaphragm, etc.
CT scan of the lungs for pneumonia
The CT scan looks different in different forms of the disease. For example, with bacterial pneumonia, images can show damage to the lower pulmonary lobes with compactions. In children, pathological lesions usually have a round shape. If the lung tissue is infected with staphylococcus, then decay cavities and pleural effusion can be seen on the images.
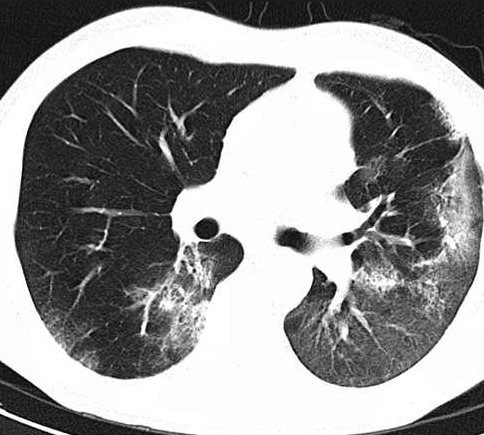
Viral lesions of lung tissue appear on images as diffusely located acinar foci, ground-glass compactions in the lung, as well as the presence of pulmonary consolidations, weakening or absence of the vascular pattern of lung tissue.
Mycoplasma pneumonia is characterized by a ground glass symptom - a hazy decrease in the transparency of the lung tissue with a pattern of blood vessels and bronchi clearly visualized against this background.
CT scan for pulmonary tuberculosis
Diagnosis of pulmonary tuberculosis should be performed not only according to CT data, but also a set of patient tests and an assessment of clinical symptoms.
The initial definition of pathology is characterized by subpleural foci in the lungs on CT images, compaction of the lung tissue like ground glass, consolidation, or a mixed nature. You can see the path to the pulmonary root, which is inflammatory in nature, as well as enlarged lymph nodes of the bronchopulmonary group.
With tuberculosis of the intrathoracic lymph nodes, the main symptom is an increase in their size. In the miliary form of the disease, multiple small foci of the lungs are visible on the images, located diffusely in all areas of the lung on CT images. In this case, differentiation from small focal metastases is required.
In the case of a focal form of tuberculosis, a few compactions are visualized on the images, which are located in one lobe of the lung, along the bronchi and in the interlobular septa. The size of the lesions does not exceed 1 cm, they can be homogeneous in structure or look like areas of increased density in the case of calcium deposition.
Optimal timing for repeating studies
If we compare thoracic tomography with conventional X-ray scans and fluorography, the total radiation field is larger. This is due to the fact that the patient takes not two projections of images, but many, and the number of scans increases several times. To obtain informative data on the entire area of the chest, the patient must remain in the field of view of the tomograph for several minutes. The longer the study, the greater the dose of radiation received at a time.
In this regard, each person is advised no more than once a year, when they can turn to tomography, but there are exceptions. CT scanning of the lungs can be repeated frequently both in case of severe diseases that require constant monitoring, and in critical situations when the expected benefit of the procedure is significantly higher than the possible harm. The following clinical situations are the reasons for repeated examinations:

- the course of the oncological process requiring monitoring;
- monitoring treatment results after surgery, chemical or radiation therapy;
- assessment of organ functionality in critical situations (trauma, stroke, heart attack, internal bleeding).
In these cases, it is better to carry out a quick diagnosis on CT than to miss important points and allow complications. Moreover, modern tomographic devices are characterized by maximum safety and reduced radiation exposure in comparison with the first generations of X-ray machines. In any case, it is always difficult to exceed the total radiation dose, even with repeated access to ionizing medical sources.











