X-ray of the calcaneus
Posted at 14:47h in Services by doctor
X-ray of the calcaneus
is the most accessible, informative and relatively safe way to study the bone and soft tissues of the foot. Such a study is often used in traumatology, surgery, orthopedics and helps to identify both mechanical damage to the heel and various congenital or acquired pathologies in this area.
- non-invasive and accurate;
- minimum radiation dose with high image quality.
When using digital X-ray equipment, images can be enlarged for a more detailed examination, and also recorded on electronic media.
What is a calcaneal x-ray?
Of all the bones of the foot, the heel is the largest. When walking, running, jumping, a large load is placed on it, which is associated with increased injuries. An X-ray examination allows you to understand how serious the heel injury is, to see whether there is a fracture and what type it is (with or without displacement).
Another common foot problem is heel spurs. It occurs due to wearing the wrong shoes, the development of arthritis or arthrosis, but most often due to formed flat feet. If this disease is not treated, it can cause complications such as heel bursitis (inflammation of the mucous bursae) and fasciitis (inflammation of the muscle tissue of the foot). The main method for diagnosing the listed pathologies is x-ray, which today can be done in almost every public or private clinic.
Indications for radiography of the heel
- Foot injury in the heel area. The causes are varied - work injury, sports injury, fracture due to an accident, and so on.
- Severe pain in the heel area. It appears mainly in the morning or after a nap, when a person, after some time of rest, gets up and rests on his heel.
- Pain in the heel area when walking.
- Changed gait (shift of the center of gravity to the toes).
- Suspicion of the development of joint diseases - arthritis, arthrosis.
- Suspicion of the presence of inflammatory diseases of bone tissue – osteomyelitis, etc.
- Suspicion of malignant and benign osteoarticular neoplasms.
X-rays are prescribed as a primary diagnostic procedure when the task is to identify the correct diagnosis and prescribe treatment. It is also carried out to monitor the condition of the heel bone, which has previously been fractured - doctors look at how correctly and quickly the bone tissue heals. Using X-rays, you can track the dynamics of various diseases of the heel bone and evaluate the effectiveness of the treatment.
What does an x-ray of the heel bone show?
Using x-rays, the integrity of the heel bone is first assessed. Then its shape and location in relation to other bones of the foot are analyzed. When identifying heel fractures, their location and direction are studied. If the fracture is comminuted, it is important to evaluate how the fragments are located and whether there is any displacement.
The image can clearly visualize neoplasms on the heel bone. In this case, their size and location are assessed, after which a conclusion is made about the possible nature of the deviation.
Using X-rays for heel spurs
A heel spur or plantar fasciitis is a pathological growth of bone tissue in part of the heel bone. This provokes discomfort, pain, difficulty in choosing shoes, trauma to the affected area and, as a consequence, further growth of bone tissue and an even greater aggravation of the problem.
X-ray therapy of the heel bone is one of the methods of treating this disease of the heel bone - under the influence of targeted irradiation, pathologically overgrown tissues are destroyed, the growth decreases. Also, due to the blockade of nerve endings, as a result of X-ray treatment, pain and inflammation are significantly reduced.
Features of the study
X-rays of the heel bone can be performed in two ways: under load and without it. In the first case, the procedure is performed in a standing position, with the patient resting on his heel. In the second case, the patient lies on his back, his legs are bent at the knees, and his feet are straight.
During the study, X-rays, passing precisely and in micro doses through an area of the human body, fall on a highly sensitive film with a special composition. The result is an image from which you can assess the condition of the bone and connective tissue of the foot and ankle joint.
An X-ray examination does not require any preparation and can be scheduled either routinely or urgently. Also, as prescribed by the doctor, an x-ray of the heel bone may be required in two projections - lateral and axial.
Contraindications for the X-ray procedure are:
- pregnancy and breastfeeding;
- circulatory disorders and bleeding;
- a critical condition of the patient, in which even minimal effects on the body can become fatal.
Interpretation of results
Immediately after the shooting, the images are developed, and the radiologist begins decoding. An x-ray allows you to find out the cause of pain and determine the nature of the pathological process. To accurately interpret the result, the doctor can compare images of healthy and diseased heels.
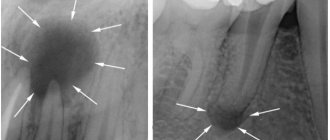
If plantar fasciitis (the so-called heel spur) is detected, the specialist gives a detailed description of the image, where he notes the presence of an osteophyte, indicating its length and location. Typically, osteophytes are visible in the image in the projection of the upper edge of the posterior tuberosity of the talus.
Symptoms of a calcaneal fracture
The first thing a patient complains about when a calcaneal bone is fractured is pain. It can occur during movement or persist at rest. Upon examination, swelling may be detected that extends to the Achilles tendon. Also among the symptoms of a fracture are: flattening and widening of the heel, hematoma in the center of the sole.
When palpating the site of injury, the patient feels sharp pain. While standing, he cannot support his injured foot.
Heel spur
Heel spur is the popular name for plantar fasciitis (more precisely, “insertional plantar fasciosis”). A widespread pathology caused by inflammation of the plantar aponeurosis at the site of its attachment to the heel bone.
Occurs with equal frequency in men and women. Provoking factors are increased body weight, decreased elasticity of the foot, limited dorsiflexion of the foot, active running and dancing.
The plantar fascia (or plantar fascia, plantar aponeurosis, plantar aponeurosis) is a thin, flat ligament that provides static support to the arch of the foot. Chronic overload of this structure leads to the formation of microtears in the area of attachment of the plantar aponeurosis to the heel bone. Repeated episodes of trauma lead to the formation of a focus of aseptic inflammation and periostitis. Since the tendons of the adductor pollicis muscle, flexor pollicis brevis, and quadratus pes are also attached to the calcaneal tubercle, their tendons may also be involved in the inflammatory process. Prolonged inflammation and periostitis can ultimately lead to the formation of ossification in the area of attachment to the heel bone, which is popularly called a “heel spur.”
It often occurs simultaneously with another pathology of the foot: apophysitis of the calcaneus, contracture of the Achilles tendon.
-Acute pain in the heel area, most often first appearing suddenly when getting out of bed.
— Initially, the pain only bothers you in the morning, often decreases when walking on your toes, but goes away as you walk throughout the day.
“Then the pain may begin to bother you in the evenings, especially after significant physical activity.
— The pain is often bilateral.
Upon inspection:
- pain on palpation along the inner surface of the heel tubercle.
- limitation of dorsiflexion of the foot due to contracture of the Achilles tendon.
- pain can be provoked by abduction of the thumb since its tendon is in close proximity to the plantar fascia.
Diagnosis of heel spurs.
X-rays most often do not reveal any changes in the initial stages of the disease. Over time, a bone spike may form, which is called a “heel spur.”

Ultrasound - allows you to identify inflammatory changes, visualize swelling and fluid accumulation around the fascial tissue.
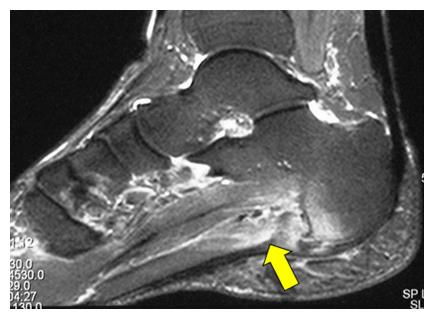
MRI is an additional research method that can be used for preoperative examination and differential diagnosis in difficult cases.
Conservative treatment is the main direction of therapy. Conservative measures consist of several main areas:
— Stretching exercises for the plantar fascia and Achilles tendon. Exercises for stretching the plantar fascia without loading with body weight are more effective.
— Wearing orthopedic insoles and shoes to relieve the plantar fascia.

- Anti-inflammatory drugs.
— Night orthosis. During sleep, a completely relaxed foot moves into a plantar flexion or equinus position. As a result, the tension of the plantar fascia weakens, and the inflammatory process leads to its scarring in a shortened position. After waking up, this causes those “morning pains”. Fixing the foot at night (during sleep) with the help of special orthoses, or simply a long stocking in a neutral position, helps prevent the scarring process with shortening of the plantar fascia.
— Plastering for a period of 2-6 weeks. Due to complete unloading in a neutral position, it allows inflammation to completely subside.
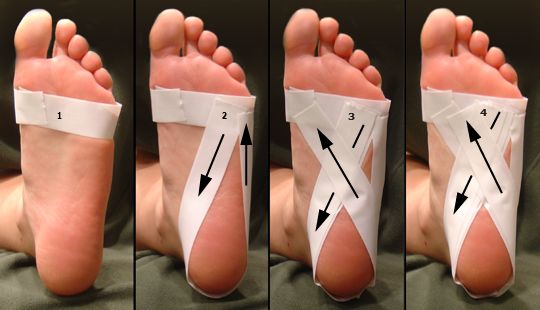
— Foot taping.
If the above measures are ineffective, more invasive interventions are resorted to over 3-6 months.
— Local injections of long-acting corticosteroids (betamethasone, diprospan). It is necessary to administer the drug only in the area of inflammation, and in a small amount, since there is a fairly high risk of atrophy of the fatty body of the calcaneus and degenerative rupture of the plantar fascia.
— Shock wave therapy. Another technology used in the fight against heel spurs. Often, several sequential procedures are required (once a month for 3 months) to achieve full clinical effect.

If all of the above methods are ineffective within 6-9 months, surgical treatment is indicated.
— Surgical release of the plantar fascia. It consists of releasing the attachment site of the plantar fascia from adhesions and dissecting its medial section into 1/3 - 2/3. It can be performed either arthroscopically (from 2 small incisions) or openly.

— In rare cases, the “heel spur” itself is removed. The indication for this intervention is its large size, which can lead to additional trauma to the plantar fascia due to bone growth itself.

— Complemented by decompression of the distal tarsal tunnel with parallel compressive neuropathy of the tibial nerve.
Surgical treatment is effective in 70-90% of cases, but is characterized by protracted rehabilitation and increased load on the outer dorsum of the foot.