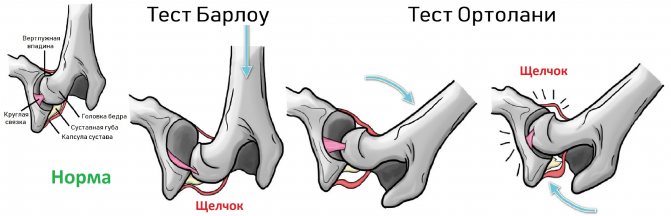
The hip joint consists of the head of the femur and the acetabulum. The acetabulum is formed by the ilium, ischium and pubis. In children, the three bones are connected by Y-cartilage. By the age of 16, the Y-cartilage ossifies, then a single innominate bone is formed.
A fibrocartilaginous articular labrum is attached to the bony edge of the acetabulum, which increases the coverage of the head and acts as a suction cup. The articular capsule is attached to the outside of the articular labrum; the head and most of the neck end up in the joint cavity.
Click on pictures to enlarge.

Congenital hip dysplasia occurs with an incidence of 6-20 cases per 1000 births. With dysplasia, the bony edge of the acetabulum is not fully developed, the head of the femur moves outward (subluxation) or extends beyond the socket (dislocation).
Due to constant friction against the hypermobile head, the articular labrum turns into a dense fibrous ring, the articular capsule is stretched and thickened. If adhesions form between the articular lip and the bottom of the cavity or the articular capsule and the ilium, reduction of the dislocation is difficult.

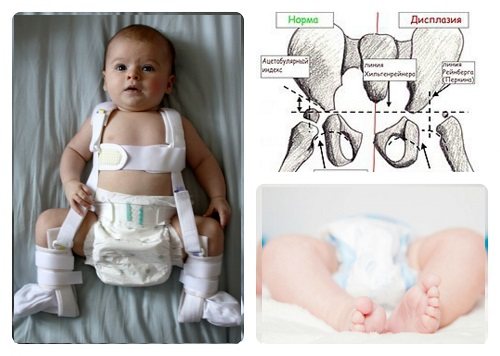
Signs of hip dysplasia: different leg lengths, asymmetry of the gluteal folds, limited hip extension. When the acetabulum is shallow, the head is easily dislocated and reduced using the Barlow-Ortolani test.
The baby lies on his back, legs bent at the knees and brought to the midline. Gently press the knee along the axis of the thigh; when it dislocates, you will hear a click. Gradually spread your legs, the reduction of the dislocation is also accompanied by a click.
The load on the bones determines their shape. If the femoral head is hypermobile or dislocated, then the bones and ligaments of the hip joint develop abnormally. Early diagnosis of congenital hip dysplasia determines the effectiveness of treatment and outcome.
Ultrasound of the hip joints in infants
In a newborn, the head of the femur has cartilaginous density, which makes it possible to evaluate the acetabulum using ultrasound. In children older than 6 months, the possibilities of ultrasound are limited due to ossification of the edges of the cavity and partially the head.
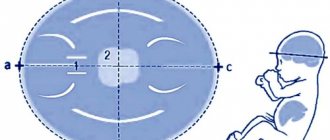
The baby lies on his back or side. The hip is assessed in neutral (15-20°) and flexed (90°) positions. A linear 7-15 MHz sensor is placed in the projection of the greater trochanter parallel (1) or perpendicular (2) to the lumbar spine.

At the first stage, the hip joint is scanned in the longitudinal plane. The main lines are drawn, the bone covering of the head, the distance from the pubic bone to the head, ∠α and ∠β are measured, and the type of structure is determined according to the Graf.
At the second stage, the stability of the hip joint is assessed using the Barlow-Ortolani test. In an unstable joint, the bone coverage of the head decreases, and the distance from the pubis to the head and ∠β increase.
At the third stage, the hip joint is scanned in the transverse plane. In cases of instability, subluxation or dislocation, the head is displaced anteriorly or posteriorly using the Barlow-Ortolani test.
Longitudinal scanning of the hip joints
The sensor is placed in the projection of the greater trochanter parallel to the lumbar spine. Find the deepest part of the acetabulum. Adjust the tilt of the transducer so that the line of the iliac shaft lies exactly horizontal (2).
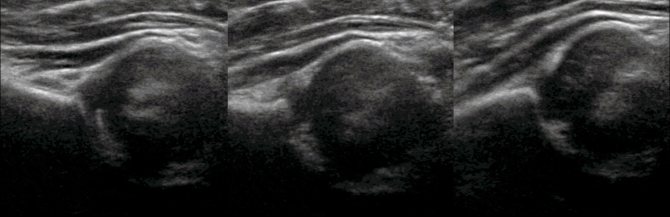
As long as the femoral head is cartilaginously dense, there is an acoustic window for examining the acetabulum. When scanning longitudinally, two photographs are documented: the first is an overview, the second is with lines and angles.

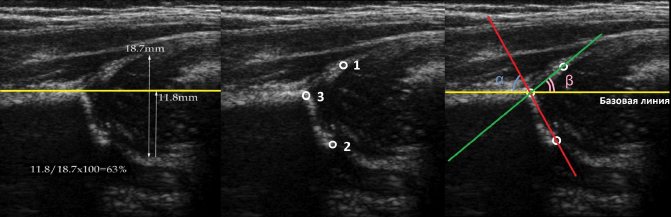
Draw a baseline along the outer contour of the ilium and mark the head of the femur, the device automatically calculates the degree of bone coverage of the head. Bone coverage of the head in cases of preluxation 40-50%, subluxation <40%, dislocation <9%.
When the head moves outward, the vacated space is filled with hyperechoic round ligament and fat. With subluxation and dislocation, the distance from the pubic bone to the head is >6 mm, the difference between the hips is >1.5 mm (3). Thick pubic cartilage is considered normal (4).

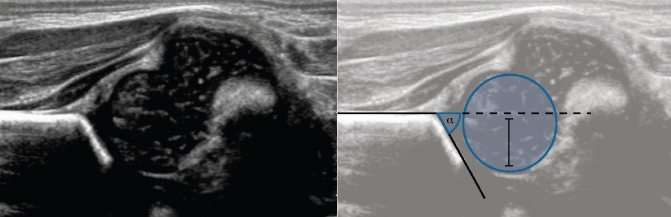
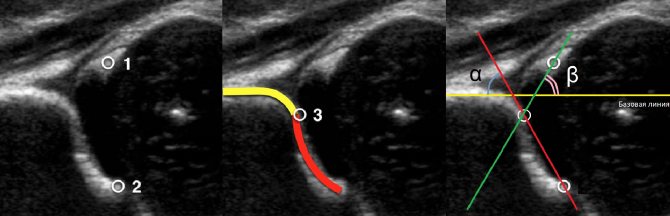
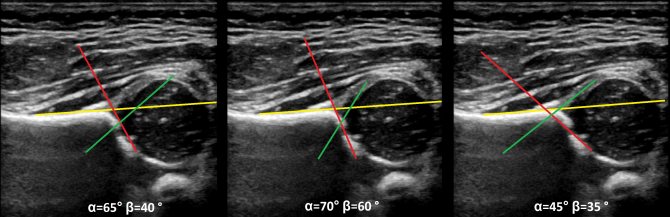
The lines of the bony (red) and cartilaginous (green) roofs pass through the bony prominence, as well as the origin of the Y-cartilage and the center of the hyperechoic tip of the labrum, respectively. The degree of development of the bone roof determines ∠α, and the cartilaginous roof ∠β.
If the edge of the ilium is rounded, the bony protrusion is determined at the point of transition of the arc of the outer contour of the acetabulum into the arc of the outer contour of the ilium. Please note that all lines follow the outer contour of the bones.
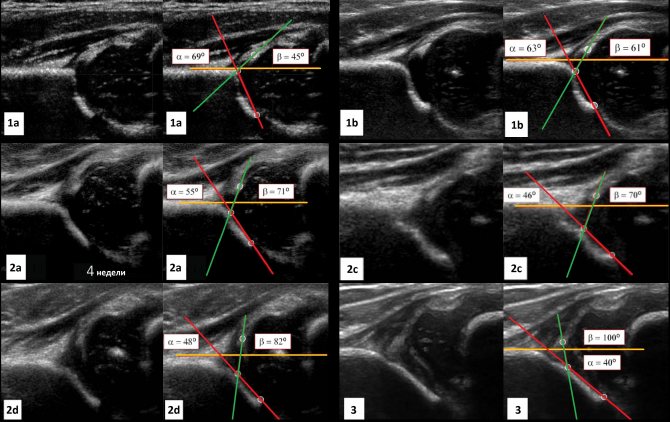
Types of hip joints according to Graf
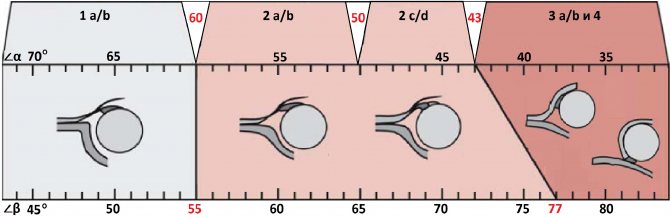
Type 1: ∠α>60°, bone coverage of the head >50%
1a : ∠β<55°. The bony roof is well contoured, the bony prominence is angular. A cartilaginous roof with a narrow base covers the head. Conclusion: Mature hip joint (type 1a). Does not require further observation.
1b : 55°<β<77°. The bony roof is well contoured. The bony prominence is slightly smoothed. A cartilaginous roof with an expanded base covers the head. Conclusion: Transient type of structure of the hip joint (type 1b). Repeat ultrasound after 3 months.
Type 2: 43°<α<59°, bone coverage of the head 40-50%
2a : 50°<α<59° in children under 3 months. The bony roof is not clearly defined. The bony protrusion is moderately flattened and rounded. Cartilaginous roof with a wide base. Conclusion: Physiological delay in the development of the hip joint (type 2a). Repeat ultrasound at 3 months.
2b : 50°<α<59° in children over 3 months. The bony roof is not clearly defined. The bony protrusion is moderately flattened and rounded. Cartilaginous roof with a wide base. Conclusion: Hip dysplasia (type 2b). Pavlik stirrups and ultrasound control once a month.
2c : 43°<α<49°, 70°<β<77°. The bony roof is flattened. The bony protrusion is rounded or flat. The cartilaginous part of the roof is expanded, but still covers the head of the femur. Conclusion: Severe dysplasia of the hip joint (type 2c), pre-dislocation. For a stable joint - Pavlik stirrups, and for instability - a plaster cast for 3 weeks, then Pavlik stirrups. Ultrasound monitoring once a month.
2d : 43°<α<49°, β>77°. The bony part of the roof is flattened. The bony protrusion is rounded or flat. The cartilaginous roof is expanded. Conclusion: Severe dysplasia of the hip joint (type 2d), preluxation (close to decentration of the head). Plaster cast for 3 weeks, then Pavlik stirrups. Ultrasound monitoring once a month.
Type 3: ∠α<43°, bone coverage of the head <40%
3a : The bony roof and bony prominence are flat. The cartilaginous roof is folded upward, the echostructure is homogeneous. Persistent decentration of the femoral head. Conclusion: Severe dysplasia of the hip joint (type 3a), subluxation. Closed reduction, then a plaster cast for 3 weeks, then Pavlik stirrups. Ultrasound monitoring once a month.
3b : Type 3b occurs in advanced forms of chronic hip dislocation. The cartilaginous part of the roof is damaged - small in size, irregular in shape, heterogeneous.
Type 4: ∠α<43°, head bone coverage <9%
The bony roof is almost flat. The head extends completely beyond the boundaries of the acetabulum. The labrum is everted or pinched between the head and the acetabulum. Conclusion: Severe dysplasia of the hip joints (type 4), dislocation. Closed or open reduction followed by a cast for 3 weeks and Pavlik stirrups. Ultrasound monitoring once a month.
Transverse scanning of the hip joints
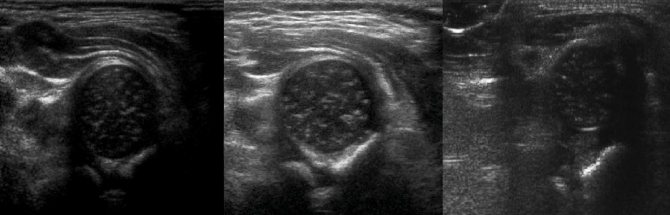
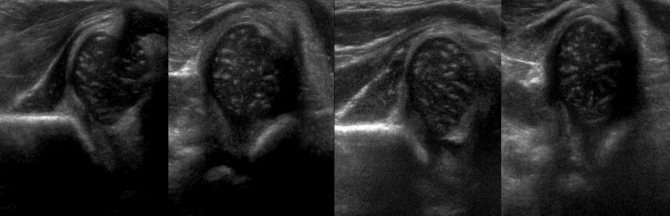
In a neutral cross-sectional position, the Y-cartilage between the ischium and pubis marks the center of the floor of the acetabulum. Normally, the center of the head passes through the Y-cartilage (1), with subluxation it shifts by 5-6 mm (2), and with dislocation the entire head is outside the socket (3).
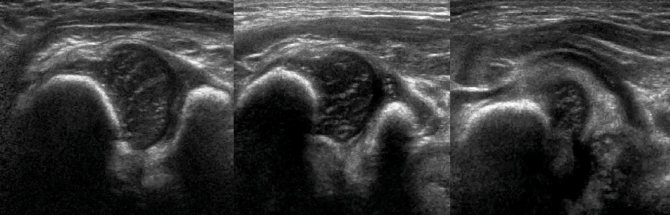
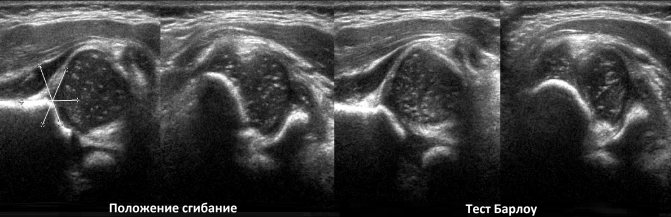
In the flexion position in the transverse section, the head is immersed in a “cup” of the metaphysis in front and the ischium in the back (1). With subluxation, the head moves outward (2), and with dislocation, it sits on top of the ischium (3).
Symptoms of dysplasia
When examining a baby, pay attention to the following signs (see photo):
- position and size of the lower extremities;
- position of skin folds in the thigh area (symmetrical or asymmetrical);
- muscle tone;
- volume of active and passive movements.
Hip dysplasia in infants manifests itself with characteristic symptoms.
- Limitation of hip abduction. Childhood hip dysplasia is manifested by limited abduction to 80 degrees or less. The symptom is most typical for unilateral lesions.
- Slipping symptom (synonym: clicking symptom). The child is placed on his back, bending his legs at both the knee and hip joints at an angle of 90 degrees (the examiner’s thumbs are placed on the inner surface of the thighs, the remaining fingers are on the outer surface). When the hips are abducted, pressure is applied to the greater trochanter, resulting in the reduction of the femoral head. The process is accompanied by a characteristic click.
- External rotation of the lower extremity is a sign characterized by outward rotation of the hip on the affected side. It can also occur in healthy children.
- Relative shortening of the limb. The symptom is rare in newborns and is observed with high dislocations.
- The asymmetrical position of the femoral and gluteal folds is revealed during an external examination.
Secondary (auxiliary) signs of hip dysplasia in a newborn:
- atrophy of soft tissues (muscles) on the affected side;
- pulsation of the femoral artery is reduced on the side of the dysplastic joint.
Asymptomatic cases of congenital hip dislocation are rare.
Tasks
Task. On ultrasound of the hip joint: ∠α=65° (1) and ∠β=60° (2). The other lines are not drawn correctly, so the angles are not correct. Conclusion: Transitional structure (type 1b) of the hip joint.
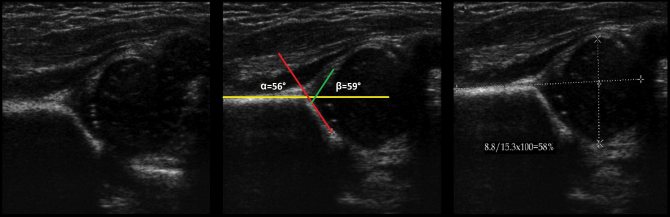
Task. On ultrasound of the hip joint: ∠α=56°, ∠β=59°; bone cover of the head 58%. Conclusion: a child under 3 months has physiological developmental delay (type 2a), and a child over 3 months has dysplasia (type 2b) of the hip joint.
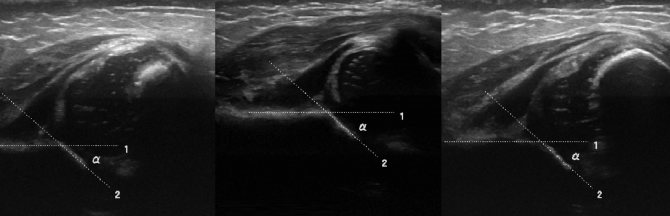
Task. On ultrasound of the hip joint: ∠α=68°, ∠β=62°; bone coverage of the head <50%. Barlow's test moves the head outward and upward - ∠β=90-93°. Conclusion: Mature (type 1b) unstable hip joint.
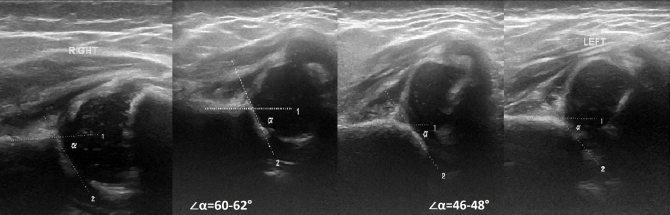
Task. Ultrasound of the hip joint: on the right ∠α=60-62°, ∠β=66-70°; on the left ∠α=46-48°, ∠β=90-93°. Conclusion: Transitional structure (type 1b) of the hip joint structure on the right. Severe dysplasia (type 2d) of the hip joint, preluxation on the left.
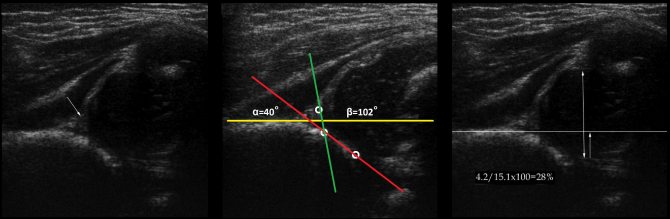
Task. On ultrasound of the hip joint: ∠α=40°, ∠β=102°; bone coverage of the head <28%. Conclusion: Severe dysplasia (type 3a) of the hip joint, subluxation.
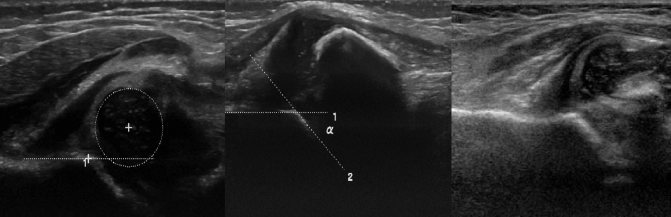
Task. Ultrasound of the hip joints, where ∠α<43°. Conclusion: Severe dysplasia (type 3a) of the hip joint, subluxation.
Task. Dysplasia of the hip joint type 4 is accompanied by dislocation: the head is displaced outward and upward, the covering of the bone roof is minimal (1); the Barlow test reveals the symptom of an empty acetabulum (2), the cartilaginous roof is wrapped inside the acetabulum and prevents reduction of the dislocation (3).
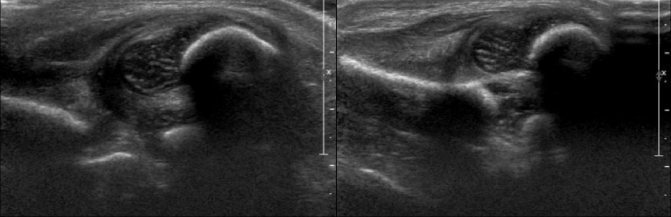
Task. Severe dysplasia (type 4) of the hip joints, dislocation on both sides. To determine the direction of femoral head displacement, evaluate the posterior and anterior margins of the acetabulum.
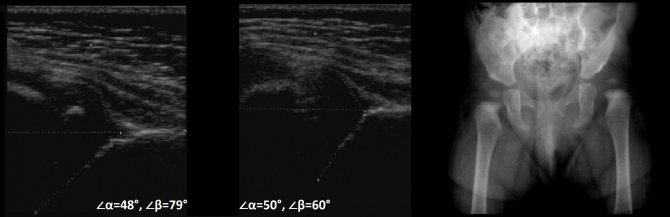
Task. A child aged 6 months, repeatedly examined by orthopedists, has excessive rotation of the left hip joint. Ultrasound of the hip joints: left ∠α=48°, ∠β=79°; on the right ∠α=50°, ∠β=60°. Conclusion: Severe dysplasia (type 2d) of the hip joint, preluxation on the left. Dysplasia (type 2b) of the hip joint, preluxation on the right. On the x-ray on the left, the head lies outside the joint - dislocation.
Task. Newborn with a positive Barlow-Ortolani test on both sides. Ultrasound of the hip joints: on the right ∠α=52°, ∠β=100°; left ∠α=49°, ∠β=95°; bone coverage of the head <9% on both sides. Conclusion: Severe dysplasia of the hip joints (type 2d), dislocation on both sides.
Take care of yourself, Your Diagnosticer !
Tags: lectures joints ultrasound