Lymph nodes are sentinels of the immune system and the zone of development of the first metastases, since these organs receive lymph with circulating cancer cells from the tissue and skin of the mammary gland. A tumor lesion of the lymphatic collector signals the spread of cancer in the body. The degree of involvement of the lymphatic system of the mammary gland determines the choice of treatment tactics and, ultimately, the prognosis for cure.
- The role of lymph nodes
- How do you know that the axillary lymph nodes have been damaged?
- How are lymph nodes affected when the tumor process spreads in them?
- Lymph nodes according to TNM classification
- Regional lymph nodes
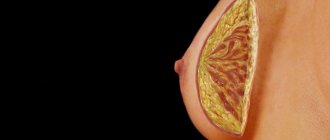
The role of lymph nodes
The lymph node (LN) is a kind of filter with a large number of various lymphocytes and other immune cells, into which the lymphatic fluid from the organs brings everything unnecessary and harmful. LNs form groups from several nodules to many dozens; lymphatic fluid flows to each group from a specific anatomical area.
Several lymphovascular pathways lead from the mammary gland to the lymph nodes of the axillary region and further to the subclavian and supraclavicular ones:
- The first and most voluminous, absorbing almost 95% of all waste lymph from the mammary gland, is the axillary path; fluid from the arm, half of the chest wall and the upper part of the abdomen also flows here. When cancer cells block the axillary lymph nodes, the fluid rushes to the lymph collectors of the abdominal cavity, which are connected by a network of capillaries with lymphoid formations in the mediastinum and ligament of the liver, introducing metastatic emboli into them.
- From the upper and posterior quadrants of the mammary gland, lymph immediately or in a roundabout way through small nodules between the pectoral muscles enters the subclavian collector, and from there flows into the supraclavicular lymph nodes to subsequently flow into the thoracic duct.
- The parasternal pathway collects fluid from the internal parts of the mammary gland and carries it to the nodules in the intercostal spaces and further to the subclavian and supraclavicular areas. The path anastomoses with intercostal lymph vessels, which are connected to the lymphatic network of the thoracic vertebrae, which explains the development of metastases in the spine.
- Lymph from the center and median lobes of the mammary gland is carried into the lymphatic system of the mediastinum, causing the formation of metastases in the lungs.
- Two interconnected lymphatic networks are formed in the skin of the breast, directing fluid into the vessels of the chest and the opposite breast, helping the spread of metastases in the skin of the chest wall.
What does MRI of lymph nodes show?
The lymphatic system is a kind of filter of the body. The most important functions are protection against toxins, infections, saturation of the blood with immune cells and nutrients. Lymph nodes are oval or ribbon-shaped formations located in groups. Normally, the organs have a uniform consistency, regular shape, and a diameter of up to 5 mm. Sizes increase as a result of immune, tumor and infectious pathologies. Identification of large nodules on MRI images may be a sign of:
- viral, bacterial, fungal diseases (HIV, syphilis, tuberculosis, etc.);
- immune pathology (lupus erythematosus, rheumatoid arthritis, etc.);
- malignant lesions of the lymphatic system (lymphogranulomatosis, etc.);
- progression of tumors of various localizations with the spread of metastases.
Scan results are not a final diagnosis. It is impossible to reliably say from the images whether the node is enlarged due to metastases or infection. The radiologist determines what the MRI shows of the lymph nodes in the neck and other anatomical areas. The attending physician makes conclusions taking into account the results of all procedures and laboratory tests performed.
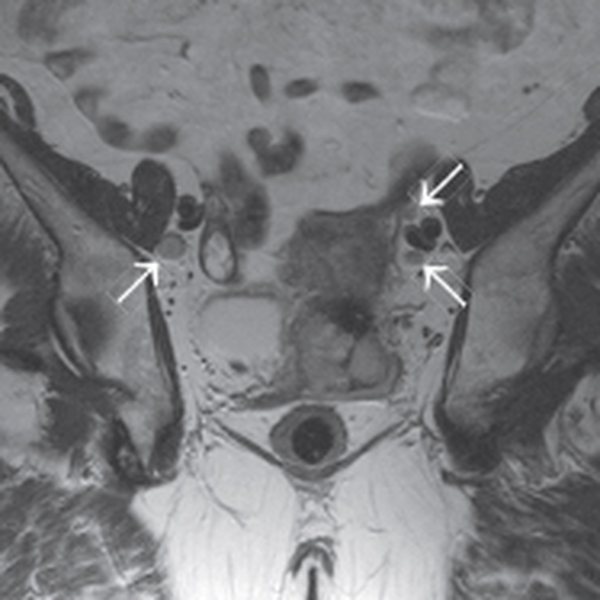
Metastatic increase in size of regional lymph nodes in cervical cancer on MRI of the pelvis (indicated by arrows), T2 VI mode in the axial plane
How do you know that the axillary lymph nodes have been damaged?
The size of a normal and healthy lymph node is from a few millimeters to two centimeters, it is soft and painless, and easily moves to the side when palpated. An increase in lymph nodes is a symptom of the inadequacy of the protective capabilities of the lymphoid organ to the health needs of the body, when the immune filter does not cope with the function assigned to it and zones of accumulation of cancer complexes are formed inside, which subsequently remain in the permanent residence.
Massive damage by metastases is easily determined by touch - the lymph nodes are large and dense, but painless and have not yet grown into the neurovascular bundle. Mammography and ultrasound of the mammary gland determine a tumor lymph node, although without taking cellular material for microscopy, this is only a “suspicion of cancer” that must be proven or rejected.
During breast surgery or before starting preoperative chemotherapy, a biopsy of the main or sentinel node, where the bulk of the lymph fluid is sent, is necessarily performed. If there are cancer cells in the sentinel lymph node, all axillary fatty tissue with everything in it is removed in one block.
How are lymph nodes affected when the tumor process spreads in them?
All removed lymph nodes, no matter how many there are in the tissue, are necessarily examined under a microscope; if there are cancer cells in them, additional studies are performed, including IHC.
The spread of cancer is believed to occur in stages: from a few cells to massive lesions, from axillary to subclavian and then to supraclavicular lymph nodes. The degrees of damage also go from minimal to maximum 3rd:
- During a morphological examination, everything pathological is detected, even cell accumulations of a fraction of a millimeter - microinvasion. The histological report will indicate рN1mic, that is, the cell complex has a size from 0.2 mm to 2 millimeters, and the letter “p” is an abbreviation for pathomorphology;
- When there is no tumor in the lymph node, the pathologist will designate the condition as “pN0”; if it is next to it (I-), then histology and IHC were performed, without immunohistochemistry - pN0 (I+);
- The next level of cancer spread through the lymphatic system is pN1 gradation, indicating a metastatic lesion larger than 2 millimeters in size, and there should be no more than three lymph nodes in the armpit;
- The pN2 lesion variant denotes a group of 4 to 9 metastatic lymph nodes in the axillary zone or a tumor in the intrathoracic lymph node;
- The final gradation pN3 suggests variations from a dozen metastatic axillary, or subclavian cancer, or involvement of supraclavicular lymph nodes.
| More information about breast cancer treatment at Euroonco: | |
| Surgeons-oncologists-mammologists | from 5100 rub. |
| Emergency oncology care | from 11000 rub. |
Classification
When determining the forms of lymphadenopathy, the location of enlarged lymph nodes is primarily taken into account. Lymphoid tissue is the main protective barrier against the spread of infectious pathogens and tumor cells. Therefore, the location of altered lymphatic formations facilitates the diagnosis of the disease that caused the lymphadenopathic reaction. Depending on the localization of the process, the following are distinguished:
- Enlargement of the submandibular lymph nodes
. Characteristic of pathological processes in the head and neck area - diseases of the eyes, ENT organs and paranasal sinuses, skin damage. Submandibular lymphadenopathy often signals dental problems and chronic tonsillitis. - Enlarged cervical lymph nodes
. Usually observed with respiratory infections, oral pathology, infectious mononucleosis, late stages of tuberculosis. Cervical nodes can be affected by lymphomas, lymphogranulomatosis, metastasis of thyroid cancer, lung cancer. - Enlarged supraclavicular lymph nodes
. Most often due to tumor causes. Detection of an enlarged node on the right is pathognomonic for cancer of the esophagus and lungs. The left lymph node is affected by malignant processes in the abdominal cavity, pelvis, and retroperitoneal space. - Enlarged axillary lymph nodes
. Inflammatory lesions are possible in the presence of wound infections, cat scratch disease, and brucellosis. Damage to the nodes of the axillary group is typical for breast cancer, melanoma of the upper extremities, and the installation of silicone breast implants. - Enlarged inguinal lymph nodes
. As a rule, nodes in the groin react to the development of syphilis, gonorrhea, chancroid, and other genital infections. Inguinal lymphadenopathy is also a sign of malignant lesions of the pelvic organs, lymphoma, and bubonic plague.
Somewhat less frequently, lymph nodes of other groups are involved in the process - submental, cubital (in the area of the elbow), parotid, occipital, jugular. During a routine instrumental examination, an increase in internal lymph nodes can be determined - intrathoracic (mediastinal), bronchopulmonary, para-aortic, splenic, mesenteric, retroperitoneal.
In the diagnostic plan, it is important to take into account other criteria for the classification of lymphadenopathy - the characteristics of altered lymphoid formations, the extent of the lesion. This approach allows us to assume the type of pathological process occurring in the involved nodes and the body as a whole. Important criteria for the classification of enlarged lymph nodes are:
- Dimensions
. With I degree lymphadenopathy, the diameter of the affected formations is 0.5-1.4 cm, with II degree - 1.5-2.4 cm, and with III degree - 2.5 cm or more. A significant and prolonged increase in the size of lymph nodes is more typical for malignant processes. - Soreness
. Intense pain is often caused by inflammation of the lymph nodes, especially acute purulent lymphadenitis. Formations that have undergone malignant degeneration are often painless, except in cases of hemorrhage into the necrotic center. - Density
_ Enlarged, inflamed lymph nodes are usually soft; when they suppurate, fluctuation (fluctuation of fluid) is felt during palpation. The stony consistency of the formations is typical for the metastatic process, and tight elasticity is typical for lymphomas. - Communication with each other
. A pathological formation of lymph nodes that can be felt as a single unit and move together is called a conglomerate. Lymph nodes fused together are detected in tuberculosis, sarcoidosis, lymphogranuloma venereum, lymphomas and metastasis. - Quantity
. It can affect either one or two or several nodes in one zone. In the first case, they talk about single enlarged nodes, in the second - about local lymphadenopathy. The more active the process, the more formations are affected, however, with metastasis, one large node is often detected. - Prevalence
. With local lymphadenopathy, single nodes are identified in one area, with regional lymphadenopathy - several formations in 1-2 adjacent zones. A generalized (widespread) process is characterized by damage to lymphatic structures in three or more areas.
Taking into account the pathogenesis, enlargement of lymph nodes can be primary (systemic), secondary (reactive) and inflammatory. Primary polyadenopathies develop with systemic malignancy of lymphoid tissue (leukemia, lymphogranulomatosis, non-Hodgkin's lymphoma) and benign processes (sinus histiocytosis). Reactive lesions are a response to another pathology (infection, immune disease, proliferation of tumor cells, metabolic disorders). Inflammation (lymphadenitis) occurs when infectious agents multiply in the tissue of the node.
Lymph nodes according to TNM classification
In the TNM system, the letter “T” denotes the primary cancer tumor, regional lymph nodes - “N”, respectively, metastases - “M”.
Metastases formed in regional lymph nodes are always only N, while cancer in the axillary region of the opposite gland is already M, as well as the lymph collectors of the neck or groin.
Clinical classification according to the degree of damage is as follows:
- N0 - lymph nodes are healthy;
- N1 - there are already metastases under the arm, but without fixation to surrounding tissues and maintaining their mobility;
- N2 - states ingrowth or dense conglomerates in the axillary zone;
- N3 - the tumor involved the subclavian or supraclavicular, or intrathoracic.
general characteristics
Enlarged lymph nodes are soft, tight-elastic or dense round formations that can be felt under the lower jaw, in the neck, axillary area, groin and other places.
The surface of the lymph nodes can be smooth or bumpy. Often the increase is preceded by acute infectious and inflammatory processes (ARVI, sore throat, pulpitis), trauma with skin damage, vaccination. Sometimes changes in the lymph nodes are detected by chance by the patient or doctor during a preventive or advisory examination. Lymph nodes are said to be enlarged when their density, surface and mobility change, and their dimensions exceed 1 cm (for elbow formations - 0.5 cm, for inguinal formations - 1.5 cm). When palpated, the nodes can be both painful and painless. In addition to lymphadenopathy, skin manifestations (elements of rash, redness of the skin), fever up to 38 ° C and above, prolonged low-grade fever, complaints of fatigue, sweating, heaviness in the left or right hypochondrium caused by an enlarged spleen and liver are possible.
The reason for contacting a doctor is the independent detection of large painless lymph nodes, sharp pain in the lymphoid tissue when trying to palpate, a combination of lymphadenopathy with other pathological signs - rash, hyperthermia, weight loss, fatigue. Particular concern should be caused by lymph nodes measuring 2-3 cm, which have enlarged for no apparent reason, are located in several zones and persist for more than 2 months.
Regional lymph nodes
Lymph nodes that collect lymph fluid directly from the mammary gland are considered regional.
The first lymphatic collector is the axillary cavity, where up to 75 lymph nodes are located at five levels from the closest to the gland to the highest at the apex, on average about three dozen. The very first and largest is the Zorgius or signal node.
The subclavian lymph nodes receive lymph from the axillary lymph nodes.
Near the sternum between the ribs there is a chain of parasternal or intrathoracic lymph nodes.
Supraclavicular lymph nodes are not regional; not so long ago, metastases in them were designated as distant, and the process was considered inoperable. Today, preoperative chemotherapy makes it possible to change the situation and perform radical surgery even in such a situation.
The equipment of Euroonko clinics and specially selected and trained medical personnel allow us to quickly provide adequate treatment according to European standards.
Book a consultation 24 hours a day
+7+7+78