Cardiotocography (CTG) is a method for assessing the condition of the fetus during pregnancy based on recording the frequency of its heartbeats and their changes.
CTG is prescribed no earlier than after the 26th week of pregnancy, since in the early stages it is not possible to decipher the data obtained. As a rule, CTG is prescribed at the 32nd week of pregnancy. By this time, the fetal rest-activity cycle and the connection between fetal cardiac activity and manifestations of motor activity are established. CTG allows you to assess the state of the cardiovascular, muscular and central nervous systems of the fetus). CTG can also be used to record uterine contractions.
When is an unscheduled CTG examination necessary?
As has already become clear, a CTG is recorded once, if the pregnant woman is not worried about anything and the doctor sees no reason to prescribe an additional examination. But there are some pathologies during pregnancy that require special attention and monitoring of the state of the fetal and uterine systems. These include:
1. The presence of a pathological version of planned tocography. Pathology of the fetal heart rate was noted. In this case, CTG is recommended to be repeated. 2. Unfavorable course of previous pregnancies. Situations when a woman’s obstetric history is burdened (miscarriages, problems with pregnancy, gestosis, fetal development abnormalities, congenital defects in previous children and other problems). This is a sufficient reason to record a CTG again, even if the current pregnancy is proceeding smoothly. 3. Situations when a pregnant woman feels disturbances in the behavior of the fetus. After all, every expectant mother feels and knows how her child usually behaves. Some children are very active and have short periods of sleep, while others sleep most of the day and are more active at night. A change in these rhythms may be a sign that the fetus is having problems. 4. Mother's illnesses. Those diseases that significantly affect the general condition of a pregnant woman, for example, influenza, acute respiratory infections, pneumonia, intestinal infections, etc. Then the need for CTG is determined by the attending physician together with the obstetrician-gynecologist. 5. The period after treatment of the fetus in utero. It is recommended to record a CTG for several weeks after inpatient or outpatient treatment. 6. Gestosis in pregnant women. This condition entails a change in the blood supply to the fetus (hypoxia). This may cause developmental delays in the unborn child. 7. Chronic infection in a pregnant woman. 8. Situations in which external factors have a detrimental effect on the fetus: smoking, alcohol and drug use by a pregnant woman. 9. Pregnant women with chronic diseases of internal organs: diabetes mellitus, coronary heart disease, arterial hypertension, obesity, chronic kidney and urinary system diseases, liver diseases, etc. 10. Post-term pregnancy.
How is the CTG procedure performed?
The fetal heart rate is recorded with a special sensor with a Doppler effect with a frequency of 1.5-2 MHz. The sensor generates an ultrasound signal that is reflected from the fetal heart, and the heart rate per minute is calculated through the heart monitor.
Before starting CTG, use a stethoscope to determine the area of best audibility of the fetal heartbeat on the anterior abdominal wall of the expectant mother, and then strengthen the sensor there. At the same time, uterine contractions are recorded using a special sensor mounted on the anterior abdominal wall in the area of the day of the uterus. Modern CTG machines have a special remote control with which a woman can herself record the movements of the fetus.
During CTG, the woman lies on a couch or reclines on a chair. The CTG procedure is quite lengthy and takes from 40 to 60 minutes. The CTG results are displayed graphically on a paper tape, which is then analyzed by the doctor and gives an opinion on the condition of the fetus.
The optimal time of day for cardiotocographic examination of the fetus is from 900 to 1400 and from 1900 to 2400 hours. It is at this time that its biophysical activity is maximally manifested.
It is not recommended to conduct CTG on an empty stomach or within 1.5-2 hours after eating. If, for some reason, the recording time is not observed, the results are considered unreliable. Because the child’s body (in utero) directly depends on the condition of the mother. After eating, glucose levels increase, which affects the activity of the fetus and its ability to respond to external stimuli.
Indications for CTG during pregnancy are:
- Preeclampsia in the second half of pregnancy;
- Maternal diseases (hypertension, diabetes, anemia and others);
- Rhesus conflict;
- Post-term pregnancy;
- Fetal growth retardation;
- Oligohydramnios or polyhydramnios;
- Multiple pregnancy;
- A burdened obstetric and gynecological history (previous abortions, miscarriages, premature births);
- Changes in the nature of fetal movements (decrease or increase in the number of fetal movements per day);
- Violation of uteroplacental or fetoplacental blood flow (diagnosis of blood flow in the mother-placenta-fetus system is carried out using Doppler ultrasound - ultrasound examination of blood flow).
Cardiotocography is based on recording the fetal heartbeat using an ultrasound sensor. Changes in the fetal heart rate during the study are recorded in the form of a graph called a cardiotocogram.
To conduct the study, an ultrasound sensor is attached to the pregnant woman's abdomen using a special tape at the point of best audibility of the fetal heartbeat. Since the fetus can lie in different ways, the sensor is attached to pregnant women at different points on the anterior abdominal wall. In case of twins, two sensors are installed simultaneously, or one fetus is examined sequentially, and then the other. Ultrasonic waves emitted by the sensor are absolutely safe for mother and unborn baby. A special transparent gel is applied to the surface of the sensor, which improves contact between the sensor and the skin of the anterior abdominal wall of the pregnant woman and the conduction of ultrasonic waves.
During the recording of a cardiotocogram, the fetal heartbeat is audible to the naked ear, which allows medical personnel and the expectant mother to monitor the correctness of the study. If the position of the fetus changes during the study and the characteristic heartbeat sound disappears, the position of the sensor changes and the study continues.
CTG is performed with the pregnant woman lying on her side or half-sitting, so that the enlarged uterus does not compress the inferior vena cava (a large vessel that carries venous blood from the lower half of the body to the heart). Compression of the inferior vena cava can lead to a deterioration in the pregnant woman’s condition, a decrease in blood pressure, and a change in pulse.
The study takes a long time: from 40 minutes to 1.5 hours. This duration is associated with periods of sleep and wakefulness of the fetus. The minimum duration of the study is 40 minutes; if during the first 40 minutes of the study the fetus falls asleep and the indicators of its condition deviate from the norm, the study will be automatically extended.
If the expectant mother gets tired of lying on one side, feels unwell, or the fetus turns in the mother’s stomach in such a way that the recording of its heartbeat is unclear, then the study can be interrupted briefly by pausing the device. If the fetus falls asleep during the study, you can “wake it up” by stroking its stomach, talking to it, or eating something sweet, for example, candy.
Attention! CTG results cannot replace a doctor’s examination and other examination methods, such as Doppler ultrasound and ultrasound.
The CTG results are interpreted by an obstetrician-gynecologist or a special program installed on the CTG device. An automated CTG assessment system allows you to accurately determine the condition of the fetus.
Types of CTG
Depending on the method of obtaining information, CTG is divided into non-stress and stress tocography (functional tests).
Non-stressful includes:
1. A non-stress test involves recording in normal intrauterine conditions of the fetus. During it, the child’s movements are recorded and noted on CTG. 2. The method of movement determines the motor activity of the fetus indirectly, by changing the tone of the uterus. It is used in the absence of a sensor that detects movement.
Stress cardiotocography (functional tests) is prescribed if the results of a non-stress examination are negative. Allows you to more deeply understand a possible problem that has arisen in the fetus and the pregnant woman.
1. Tests that simulate the birth process: - Stress oxytocin test. Contractions are induced by intravenous administration of the hormone oxytocin and the response of the fetal heartbeat to moderate uterine contractions is monitored. — Test with nipple stimulation (mammary test). With this technique, contractions are stimulated by irritation of the nipples. The pregnant woman herself causes irritation until the moment when contractions begin. This moment will be visible from the cardiograph readings. This method is safer compared to the previous one. It also has significantly fewer contraindications. 2. Tests affecting the fetus: - An acoustic test allows you to determine the reaction of the fetal cardiovascular system in response to irritation by sound. - Palpation of the fetus - a slight displacement of the presenting part of the fetus (pelvis or head) is performed above the entrance to the pelvis. — Functional tests that change the parameters of the blood flow of the fetus and uterus. Today they are practically not used.
How is fetal CTG performed?
No special preparation is required to conduct CTG after thirty weeks. It is recommended to do the study during periods of greatest fetal activity, from nine in the morning to two in the afternoon, and from seven in the evening to midnight. It is not advisable to perform CTG on an empty stomach, as well as on a full stomach or immediately after the administration of glucose. The optimal time is an hour or an hour and a half after eating.
There are two different types of CTG during pregnancy - direct and indirect. Direct cardiotocography is rarely performed and only during childbirth when the integrity of the fetal bladder is damaged. It is done using a special spiral-shaped needle-shaped sensor, which is inserted into the presenting part of the fetus. Uterine tone is measured using a catheter that is inserted into the uterine cavity. Indirect fetal CTG is done through the anterior abdominal wall. Two sensors are used - one is attached in the place of best audibility of the heartbeat (the doctor determines it with a stethoscope before the examination), the other - in the right corner of the fundus of the uterus.
CTG is performed with the woman sitting or on her right side. It is not recommended to lay a pregnant woman on her back, as this may compress the main blood vessels and the CTG reading will be incorrect. The average procedure time is 40 minutes. If the fetus has a normal rhythm, CTG can be reduced to 15-20 minutes. During childbirth, the duration of the study should be at least twenty minutes, or five contractions.
The first ten minutes measure the basic rhythm, such a fetal CTG is called non-stress. It is supplemented by recording fetal movements (using a sensor or according to the pregnant woman). Then they move on to functional tests or stress CTG. The following tests are used to study the baby's heartbeat in the womb:
- Oxytocin test
- Mammary test
- Acoustic test
- Fetal palpation
- Reflex tests
The oxytocin test is carried out mainly before childbirth and in a hospital setting. With the help of oxytocin, contractions are provoked in a woman and CTG of the fetus is performed with increased contractions of the uterus; examination is rarely performed. The mammary test is essentially similar to the oxytocin test, but safer. The pregnant woman stimulates the nipples with her fingers, which causes increased uterine contractions. The test is contraindicated in case of increased tone and threat of premature birth. During an acoustic test, CTG records changes in the fetal heartbeat when exposed to a sound stimulus. During palpation of the fetus, its presenting part is slightly displaced. Reflex tests are rarely done. Functional tests that change the parameters of placental blood flow and the atropine test are no longer used.
CTG during pregnancy can be performed using different equipment. Previously, most clinics used devices that recorded heartbeats and uterine contractions on paper; the doctor did the decoding himself. This required high qualifications and experience of a specialist. Nowadays, equipment with computer decoding is increasingly used, this allows one to obtain more reliable results. There are also opportunities to conduct CTG weekly online. Special sensors are attached to the skin of the abdomen, the signal is transmitted via a smartphone to a computer monitor, where the doctor is able to monitor changes in the fetal cardiac activity.
Main indicators of CTG
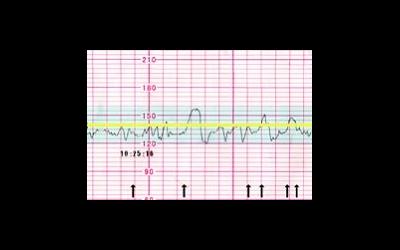
Basal rhythm (BHR or HR) is the average heart rate. Normally it is 110-160 beats per minute in a calm state, 130-190 during fetal movements. Heart rate should not go beyond the normal range and be smooth.
Rhythm variability (heart rate range) is the average deviation of the rhythm from the basal one. Normally it ranges from 5 to 25 beats per minute.
Acceleration – peak of heart rate acceleration (looks like tall teeth on the graph). Normally – 2 peaks per 10 minutes during the period of fetal activity. Amplitude – 15 beats per minute.
Deceleration is a slowdown in heart rate (looks like depressions on the graph). Normally, they should be absent or quick and shallow. The number of decelerations should tend to zero, the depth should not exceed 15 beats per minute, and there should be no slow decelerations at all.
Fetal condition indicator (FSI) is normally less than 1, from 1 to 2 - minor violations, more than 2 - obvious violations.
The tocogram shows the activity of uterine contractions. Normally, uterine contractions should be no more than 15% of the BHR.
What is CTG?

Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.
Cardiotocography (CTG)
is a method of functional assessment of the condition of the fetus during pregnancy and childbirth based on recording the frequency of its heartbeats and their changes depending on contractions of the uterus, the action of external stimuli or the activity of the fetus itself.
CTG is currently an integral part of a comprehensive assessment of the fetal condition, along with ultrasound and Doppler. Such monitoring of fetal cardiac activity significantly expands diagnostic capabilities both during pregnancy and childbirth, and makes it possible to effectively resolve issues of rational tactics for their management.
Fetal cardiac activity is recorded with a special ultrasound sensor with a frequency of 1.5 - 2.0 MHz, the operation of which is based on the Doppler effect. This sensor is mounted on the anterior abdominal wall of a pregnant woman in the area of best audibility of fetal heart sounds, which is previously determined using a conventional obstetric stethoscope. The transducer generates an ultrasound signal that is reflected from the fetal heart and again sensed by the transducer. The electronic heart monitor system converts recorded changes in the intervals between individual fetal heartbeats into the instantaneous heart rate of the fetus, calculating the number of beats per minute at the time of the study.
Changes in heart rate are displayed by the device in the form of light, sound, digital signals and a graphic image in the form of a graph on a paper tape. Modern CTG devices provide a special remote control with which a pregnant woman can independently record the movements of the fetus. Contractions of the uterus and fetal movements are displayed by the device during the examination at the bottom of the paper tape in the form of a curved line.
When performing CTG, simultaneously with recording of the fetal cardiac activity, the contractile activity of the uterus is recorded with a special sensor, which is fixed on the anterior abdominal wall of the pregnant woman in the area of the uterine fundus. When deciphering a CTG recording and assessing the relationship of the obtained data with the condition of the fetus, one should proceed from the fact that the resulting recording reflects, first of all, the reactivity of the fetal nervous system and the state of its protective and adaptive reactions at the time of the study.
Changes in the fetal cardiac activity only indirectly indicate the nature of the pathological processes occurring in the fetal body. However, the results obtained from analyzing the CTG recording cannot be identified only with the presence of varying degrees of oxygen deficiency (hypoxia) in the fetus. Below are a few of many possible examples that support this idea.
Fetal hypoxia and cardiotocography (possible interpretation errors)
- Fetal hypoxia is most often caused by a decrease in oxygen delivery to the uteroplacental bloodstream and dysfunction of the placenta. In this case, the response of the fetal cardiovascular system occurs, accordingly, due to the presence and severity of a decrease in fetal blood oxygen saturation. A clear disturbance in the condition of the fetus will be reflected accordingly in the CTG recording.
- In some cases, a relatively short-term disruption of blood flow in the vessels of the umbilical cord is possible, for example, due to their pressing by the fetal head. This phenomenon will also be reflected in the nature of the CTG recording, as if giving it a pathological character, although, in fact, the fetus does not suffer. This creates a false illusion that the condition of the fetus is impaired.
- As a protective reaction, the fetus may decrease tissue oxygen consumption and increase resistance to hypoxia. The CTG recording will be normal, despite the fact that the fetus is experiencing hypoxia. It’s just that the situation is still compensated.
- In various pathological conditions, it is possible to reduce the ability of tissues to perceive oxygen when its content in the blood is normal, which may not cause an appropriate response from the fetal cardiovascular system, despite the fact that the fetal tissues lack oxygen and the fetus suffers. Those. in such a situation, the CTG recording will be normal, despite the disturbance in the fetal condition.
Thus, CTG is just an additional instrumental diagnostic method, and the information obtained as a result of the study reflects only a small part of the complex changes occurring in the mother-placenta-fetus system. The information obtained from a CTG study must be compared with clinical data and the results of other studies, since two similar records with almost the same diagnostic characteristics can have completely different diagnostic value for different fetuses.
Conditions for obtaining reliable information about the condition of the fetus based on CTG data
Cardiotocographic examination is carried out with the pregnant woman lying on her back, on her left side, or sitting in a comfortable position.
CTG can be used no earlier than 32 weeks of pregnancy. By this time, a relationship is formed between cardiac activity and the motor activity of the fetus, which reflects the functionality of several of its systems (central nervous, muscular and cardiovascular). By the 32nd week of pregnancy, the formation of the fetal activity-rest cycle also occurs. In this case, the average duration of the active state is 50-60 minutes, and the calm state - 20-30 minutes. Earlier use of CTG does not ensure diagnostic reliability, as it is accompanied by a large number of false results.
Of primary importance in assessing the condition of the fetus is the period of its activity. It is important that during the CTG, at least part of the period of fetal activity, accompanied by its movements, is recorded. Taking into account the calm state of the fetus, the required total recording duration should be 40-60 minutes, which minimizes the possible error in assessing the functional state of the fetus.
On the one hand, there is an opinion that CTG is insufficiently informative in diagnosing fetal disorders, as evidenced by a considerable number of false-positive results in the group with pathological changes on the cardiotocogram. According to other data, the accuracy of the prediction of the satisfactory condition of newborns coincided with the results of CTG in more than 90% of cases, which indicates the high ability of the method to confirm the normal condition of the fetus. However, in fact, the informativeness of the method largely depends on the method of interpreting the data obtained during the study.
Decoding the cardiotocography recording
When deciphering the CTG recording, a number of indicators are determined that have normal and pathological signs, which make it possible to assess the state of reactivity of the fetal cardiovascular system. In a number of cases, methods of computer evaluation of CTG recordings are used. So, in particular, when interpreting CTG data, they use the calculation of the fetal condition indicator - PSP. In this case, PSP values of 1 or less may indicate the normal condition of the fetus. PSP values of more than 1 and up to 2 may indicate possible initial manifestations of fetal impairment. PSP values of more than 2 and up to 3 may be due to the likelihood of severe disturbances in the condition of the fetus. A PSP value of more than 3 indicates a possible critical condition of the fetus. Various scales for assessing CTG indicators in points are also widely used.
Among them, the most common are the scales proposed by W. Fischer et al. (1976), E. S. Gauthier et al. (1982), as well as their various modifications. In this case, a score of 8-10 points corresponds to a normal CTG; 5-7 points is suspicious and may indicate initial manifestations of fetal impairment; A score of 4 or less may indicate significant impairment in the condition of the fetus.
However, these indicators should be treated very carefully and differentiated. It should be understood that the conclusion based on the interpretation of the CTG recording is not a diagnosis.
, but only provides some additional information along with other research methods. The results of a single study provide only an indirect idea of the condition of the fetus from the moment of the study for no more than a day. Due to various circumstances, the nature of the reactivity of the fetal cardiovascular system can change in a shorter time. The severity of disturbances in the reactivity of the fetal cardiovascular system may not always coincide with the severity of the disturbance in its condition. The results obtained should be considered only in relation to the clinical picture, the nature of the pregnancy and data from other research methods, including ultrasound and Doppler.
Safe fetal monitoring
However, the CTG method has no contraindications and is absolutely harmless. Based on this, the use of CTG during pregnancy allows monitoring the condition of the fetus over a long period of time, and if necessary, this can be done daily, which significantly increases the diagnostic value of the method, especially in combination with data from other diagnostic methods.
CTG is also successfully used during childbirth, which makes it possible to monitor the condition of the fetus during labor and evaluate uterine contractions. CTG data facilitates assessment of the effectiveness of treatment during labor and, often, the results of the study are the reason for changing the tactics of labor management.
Ideally, every woman's birth should be controlled by CTG. Particular attention should be paid to premature and delayed labor, excitation and stimulation of labor, childbirth with breech presentation, as well as childbirth with fetoplacental insufficiency and fetal hypoxia.
The results of CTG during childbirth are also assessed strictly individually and only in combination with clinical data, as well as with the results of other studies conducted on the eve of or during childbirth.
Ultrasound scanner WS80
An ideal tool for prenatal research.
Unique image quality and a full range of diagnostic programs for an expert assessment of a woman’s health.
Problems that CTG helps to identify
1. Entanglement of the umbilical cord or its compression, which subsequently causes a decrease in the supply of oxygen to the fetus from the mother.
In addition, sufficient nutrients will not be delivered through the blood. All this affects the growth and development of the fetus. 2. Violation of fetal heart rhythm. Irregular heartbeat can occur in the presence of defects and stigmas in the development of the cardiovascular system of the unborn child. 3. The fetus experiences hypoxia. Even a slight disruption in the delivery of oxygen or nutrients through the umbilical cord blood will be recorded on CTG. In cases where, after performing a CTG, the doctor notices deviations from the norm, the woman may be prescribed additional ultrasound and Doppler sonography. Sometimes you need to undergo a course of treatment and repeat the examination over time.
Errors in CTG recording that distort the result
There are a number of situations when pathological changes are recorded on a CTG recording in an absolutely healthy woman and fetus.
1. Overeating before the examination. 2. Recording made while the child is sleeping. 3. Maternal obesity. Through a significant layer of subcutaneous fat, it is difficult to listen to the fetal heartbeat. 4. Excessive physical activity of the child. 5. Situations involving insufficiently tight fit of the sensors, or drying out of the special gel. 6. Multiple pregnancy. Recording the heartbeat of each fetus individually is very problematic.