Treatment of caries, is it painful to treat?
Caries is a slow-moving pathological process occurring in the hard tissues of teeth, which develops due to the influence of certain external and internal factors.

At the initial stage of development, caries is characterized by focal demineralization of the inorganic part of the tooth enamel and its gradual destruction, affecting the organic matrix, as a result of which this leads to a violation of the integrity of the hard tissues of the tooth with the formation of cavities in the dentin, and in the absence of timely treatment - to the occurrence of inflammatory complications with side of the pulp, leading to periodontitis.
Treatment of caries is completely painless, since all dental procedures are performed under complete anesthesia.
Prices for treatment of caries of anterior teeth in Moscow
The price for treating caries of anterior teeth largely depends on the technique used. Standard therapy with the installation of a light filling will cost from 5,800 rubles. But prices for restoration start at 12,500 rubles. Treatment costs approximately the same without an Icon drill. Treatment of pulpitis on the front teeth involves cleaning the canals, which will add several thousand more to the total amount. If the tooth is seriously damaged and installing a filling is impossible, get ready for serious expenses. The average cost of a ceramic crown is from 25,000–30,000 rubles, and turnkey implantation will cost at least 55,000–100,000 rubles for the installation of one implant.
Development of caries
With the development of the carious process, slow tooth destruction occurs, beginning with a decrease in the amount of mineral substances that make up the tooth enamel, as a result of which a carious cavity (hole) is formed in the tooth.
Tooth decay can occur at any age; its prevalence reaches almost 100 percent
Caries is the most common human disease. In childhood, this pathology occupies a leading place among all diseases and occurs almost 10 times more often than the second most common human disease - bronchial asthma. According to various sources, up to 90% of children with baby teeth and about 85% of adolescents at the time of leaving school have carious cavities to one degree or another in disrepair. 98% of adults have dental fillings.
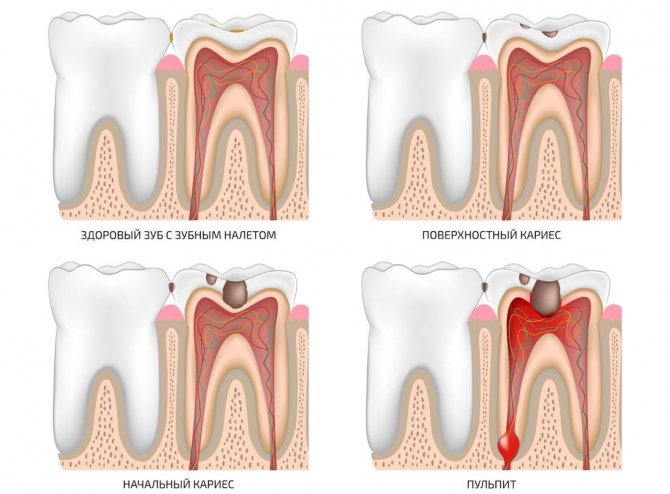
Types of caries: a visual demonstration
Caries is a disease that damages the hard tissues of the tooth: enamel and dentin. When the enamel is initially damaged, the carious area usually becomes milky white and loses its shine. When it comes to dentin, by this time both areas of porous demineralized enamel and locally the dentin itself usually already look brown or even almost black, as they are colored by various substances, including food dyes.
Thus, the stage of the disease, the nature of its course and the localization of the lesion complement the picture and determine exactly what caries looks like on the teeth: color, size of the damage, depth of the carious cavity, number of lesions, etc.
For example, in the photo below there is fissure caries. On teeth, it appears on the chewing surface in natural depressions called fissures. In some cases, the black lines turn out to be so small that the dental probe and the doctor’s gaze do not linger on them, but often the problem is clearly visible to the naked eye:

Fissure caries is dangerous because large areas of damaged dentin can be hidden under seemingly minor damage to the enamel. For a better understanding, watch the video, which schematically shows how caries penetrates into the deep tissues of the tooth:
Interesting information about the structure of the tooth and its damage by caries
And this photo shows another example of what teeth affected by generalized caries can look like. This is a very dangerous form of the disease, which threatens a person with the loss of a significant part of the teeth, depulpation (removal of nerves) and the installation of crowns:

In appearance and the nature of its course, bottle caries is close to generalized. The main difference between these diseases is the age of the people they affect: bottle caries develops mainly in children from 1 to 3 years old. This is often due to weakened immunity and somatic diseases of early age.
Photos of bottle caries:

A note about bottle tooth decay
The causes of bottle caries go far beyond feeding a child milk, especially before bedtime, as some parents think. What is important here is: violation of the feeding regime, non-compliance with hygiene rules by parents in relation to baby teeth, the factor of systemic diseases of the baby, aggravating the background of carious processes, directly and indirectly affecting the already formed and not yet fully mineralized enamel lattice, the composition of the baby’s saliva is also important. In general, we cannot limit ourselves to one definition of “a bottle of milk - caries”.
A separate form is recurrent caries, which appears on previously cleaned surfaces. It usually develops at the site of poor-quality tooth treatment around the filling. In the later stages of development, tissues affected by caries frame the filling and are clearly visible to the naked eye.
It is also useful to read: What is important to know about caries of primary teeth in young children
The photographs show how caries develops under the filling, manifesting itself in the places where it adheres to the surrounding tooth tissues:

Another type of hidden caries is caries under the gum, where it affects the cementum of the tooth root. For this reason, it is also called root caries or cement caries. It develops faster than caries of exposed areas of enamel, but it is very difficult to see.
The photo below shows an extracted tooth with root caries:

If the disease develops in the cervical area of the tooth, that is, in areas close to the gum, then in this case we are talking about cervical caries. This pathology also has a characteristic appearance: at the base of the tooth it appears as if it has been sharpened, sometimes along the entire perimeter, while the upper part of the crown often remains completely intact.
The following photographs show several examples of cervical caries:

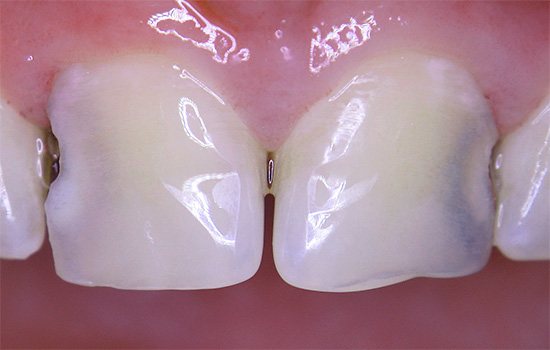
Approximal caries (sometimes simply called interdental caries) is very difficult to detect: it develops on the surface of the tooth in contact with the wall of the neighboring one. Due to the difficulty in fully cleaning the interdental space with a toothbrush, such caries can erode the enamel and then the dentin for a long time and imperceptibly, often leading to the fact that a person seeks help already at the stage of deep carious tooth damage.
An example of approximal (interdental) caries - note that it is practically invisible:

But in the case of a strong growth of the carious cavity between the teeth, such caries looks quite, so to speak, classically:
It is important to note that, although in most of the above photos with dental caries the disease is shown at fairly late stages of development, when damage and staining of dentin has begun, this does not mean that caries necessarily means brown or black spots and holes in the teeth. The color of the affected areas depends on the stage of development of the disease, and can vary greatly, ranging from snowy white to black, including all kinds of variations of brown, gray and yellow.
Symptoms of caries
Caries begins to be felt as a sudden, acute pain when cold, hot, sweet or sour food comes into contact with a carious tooth. In this case, the patient feels severe, often unbearable acute pain. At the same time, a soft plaque forms on the teeth and the viscosity of saliva sharply increases.
With the development of microorganisms in the oral cavity, a so-called dental plaque (soft plaque) is formed, which, under certain conditions, is fixed on the surface of the tooth. The microflora of dental plaque, in turn, destroys the basis of tooth enamel and in the resulting carious defect, microbes are subjected to enzymatic breakdown of the organic matter of the tooth.
After some time, with specifically located affected areas of the tooth after the onset of caries development, patients can visually observe open carious cavities (holes in the teeth), but sometimes this does not happen, the patient does not see carious cavities if these cavities are located on the inner surfaces of the teeth or in other hard-to-reach areas. for self-examination of places, for example, located close to the root of the tooth or covered by the gum.
White caries - black caries, time plays against teeth
The enamel is translucent and normally ranges in color from light yellow to grayish-white. The color of dentin and any material underneath the enamel greatly affects the appearance of the tooth. Surprisingly, caries begins in the form of the formation of a barely noticeable white matte spot on the enamel (Fig. 6) [3].
Figure 6. “Dental problems.” Over time, the white spots on the enamel caused by caries darken.
drawing by Anastasia Prokhorova
Further, such a stain darkens from frequent meals: the area of the tooth softens more and more, and in the lucky ones a painless hole is formed - a carious cavity [7]. For some unfortunate people, caries is accompanied by inflammation of the tissues around the tooth, infection, and sometimes even an abscess, which can lead not to the small aesthetic problem of “black spots”, but to the loss of the tooth itself.
Caries, statistics
Data from various studies indicate that in equatorial regions (Africa, Asia) caries is less common than in the northern and polar regions (Scandinavia, North America). People living in developing countries also have a higher incidence of dental caries, but in this case this is not due to genetic predisposition or the influence of external factors, but to a much lower availability of dental care than in developed northern countries.
Caries is of infectious origin associated with the activity of microorganisms such as veyonella, lactobacilli and other microbes. Streptococci play a leading role in the development of dental caries disease.
A decrease in resistance to caries is associated with a decrease in the calcium content of tooth enamel, with a decrease in the calcium/phosphorus ratio, as well as with immune disorders in general. Researchers associate the decrease in the body’s immunity mainly with a decrease in the content of secretory immunoglobulin type “A” in saliva, which prevents the attachment of microorganisms to the surface of tooth enamel and thereby prevents the formation of soft plaque, which, with insufficient hygiene, is susceptible to hardening and the formation of hard tartar.
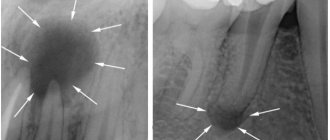
Is it caries or pulpitis visible in the picture?
There is a picture of an orthopantomogram. Can you use it to determine whether there is caries in a tooth or pulpitis? In general, I don’t want my tooth to be picked, because if there is caries, I will treat it right away, and if there is pulpitis, then after the holidays. The tooth doesn't hurt. Or will they also tell you to take a targeted photograph of this tooth? And I did ortho a month ago, is it possible to take another shot now?
It’s obvious, but this pulpitis needs to be treated immediately, it can turn into more serious things, especially since on vacation you won’t know where to run.
In this section, only neutral information is published in topics and comments. Topics and comments containing advice, recommendations, promotion of alternative methods of treatment or other actions will be closed.
The picture is always ambiguous, since it is an orthopantomogram, then in the picture you can only see a slice, one of many. The fact that the tooth does not hurt is of course good, but it happens that with chronic pulpitis there is no pain. Therefore, just take the time and go get a tooth if you don’t want to take a 3D photo. And find a doctor you trust, because as a rule, a good specialist doesn’t really want to dig into the canals of a tooth and treat pulpitis if it’s caries (that is, he won’t lie for the sake of making money), because root canal treatment is a complex, painstaking job, where there can be many complications. And now the patients are gone...legally literate) I’ll summarize: examine your tooth if it hasn’t darkened, if it doesn’t react to cold/hot, and if it doesn’t hurt when tapped. This means you can still get by with caries. A snapshot in such borderline conditions may be mistaken.
Treatment of caries
Treatment of caries in the Lyubertsy dental clinic "VUGI" begins with an examination of the oral cavity by a dentist, a thorough diagnosis of the condition of all teeth with mandatory mechanical treatment of detected carious cavities. Mechanical impact is carried out using special systems using boron. After mechanical treatment of the carious cavities, medications are used, after which the carious cavity is filled with one or another filling material.
It is impossible to overestimate the importance of timely contacting a dental clinic for caries treatment. Patients should know that there is no difference between the extent of dental caries damage and the intensity of pain.
It is because of ignorance of this fact that patients get an appointment with a dentist with already severely advanced caries, when longer and more complex treatment and a large number of repeat visits are already required, which is especially offensive, since visits to a dentist-therapist require a fairly large amount of time ; In addition, this fact always leads to additional monetary costs.
In the initial stage of the disease, if such a possibility exists, non-operative treatment of caries consists of carrying out comprehensive professional oral hygiene; during these manipulations, the dentist removes plaque and restores the affected enamel. Such manipulations are carried out through the use of fluorides in the form of solutions, pastes, gels, and varnishes. Often such doctor’s actions are combined with the use of solutions of calcium salts and restorative drugs.
In acute forms of caries, the patient is prescribed a special diet rich in proteins and mineral salts and vitamins A, C, D. Calcium preparations are also prescribed, such as colecalciferol, calcinova, calcium carbonate, sodium fluoride.
Timely diagnosis of caries using panoramic images
Problem: the patient came to the Family Dentistry with complaints of periodic pain in the teeth on the lower right. The patient could not indicate a specific tooth, but assumed that the wisdom tooth on which he saw a dark spot was to blame.

Solution: a panoramic photograph of the teeth was taken for diagnosis. Caries of three teeth was discovered and treated: one of the teeth was depulped, tooth canals were treated with a microscope and restored with a ceramic inlay, the other two teeth were restored with light fillings.

A situation similar to that considered in this work occurs quite often. The patient either cannot indicate the exact source of the pain, or points to a tooth that doctors do not consider problematic. Dial-Dent specialists have extensive experience in finding the cause of unclear pain in the teeth (see the work “Pain in a tooth, but not that one...”). A huge help in correct diagnosis is a modern digital orthopantomograph, with the help of which Dial-Dent takes a panoramic photograph of the teeth. A panoramic shot allows you to see the whole situation and find out where the source of pain lies. Correct diagnosis using modern digital equipment saves the patient time, effort and money. A digital panoramic image is clearer, and the doctor can enlarge individual fragments for a closer look. All this, as well as more than 10 years of experience of Dial-Dent specialists, makes it possible to conduct high-quality diagnostics, and as a result, precise targeted treatment, quickly relieving the patient of dental pain.
Classification according to the depth of the carious process
For a dental therapist involved in the treatment of caries, a topographic classification is more convenient:
- spot stage caries;
- uncomplicated simple caries;
Stain stage caries is the first stage of caries, in which the tooth enamel changes its color due to the formation of a so-called chalky stain on it. At the same time, the tooth remains smooth, since the enamel is still only in the initial stages of destruction. When diagnosing this stage, the most important task of the dentist is to stop the further development of the disease and its transition to the next stages of development.
In the earliest stages of caries, its therapy is considered a fairly simple task, is practically painless, takes a minimum of time (only one visit to the dentist is possible) and, accordingly, the least expensive. At the initial stage of caries, the dentist begins treatment of the tooth with the procedure of removing the stain, after which the enamel is remineralized, while the following preparations are applied to the neck of the tooth: sodium fluoride solution, calcium gluconate and others. Dentists can also use techniques such as infiltration-impregnation.
Superficial caries in the initial stage
At the stage of superficial caries, the surface of a timely undetected and unremoved chalk stain becomes rough due to demineralization of the enamel. In this case, the enamel-dentin junction of the tooth is not yet affected. The tooth at the site of superficial caries begins to hurt from cold food or hot food and may become sensitive to sweet or sour foods.
Treatment for this stage of caries will usually involve grinding down the area of the tooth. After grinding, just as in the case of the treatment of the previous, very first stage of caries, remineralizing therapy is performed.
But, in cases of caries localization in the fissures or on the contact surfaces of the teeth (these areas are the most susceptible to caries, since there are good conditions for food sticking and they are difficult to access for cleansing), then rem therapy becomes ineffective, so the dentist needs to prepare the affected area according to the classical method followed by filling. Superficial caries must be distinguished from such non-carious diseases as erosion of hard tissues and wedge-shaped defects.
Average caries
At the stage of average caries, the lesion begins to penetrate deeper. The enamel-dentin junction is affected, and the dentist can easily determine the deep pathology of the tooth. With average caries, the patient often feels pain, which becomes longer and more intense; pain, as a rule, occurs in the evening and at night, as a result of which the patient’s quality of life suffers greatly. Treatment of caries that has developed to a moderate form consists of removing the damaged part of the tooth and treating it with medications, followed by installing a filling of the desired type.
Deep caries
When, with advanced untreated caries, damage reaches the peripulpal dentin, the stage of deep caries begins. Therapy for deep caries consists of complete removal of the carious part of the tooth, followed by treatment of the damage with medications, the use of remineralizing drugs and filling. In the absence of treatment or inadequate therapy for this pathology, after the destruction of dentin, damage to the pulp occurs - pulpitis, which turns into periodontitis.
Complicated caries (pulpitis, periodontitis)
This classification takes into account the depth of the lesion, which is a determining factor for the choice of treatment method.
Caries in the initial stage (spot stage), superficial caries, medium caries with small defects are not detected on an x-ray. At the same time, it is very important to differentiate caries from other dental pathologies; for example, caries in the spot stage must be separated from such non-carious lesions as hypoplasia and fluorosis.
What these pathologies have in common is the formation of stains on the teeth, EOM (electroodontometry) readings are normal, and the absence of any discomfort. What are the differences: caries, unlike these two pathologies, can be detected when stained with special dyes, fluorosis and hypoplasia occur before teething, and caries always occurs after; caries is found in caries-susceptible areas, and non-carious pathologies in atypical (caries-resistant) areas.
Radiation diagnostics of proximal caries
The most difficult to detect is proximal caries (caries dentis proximalis), that is, a process localized on the contact surfaces of the tooth, considered proximal relative to the contact point. It is these lesions that most often remain unrecognized during routine examination.
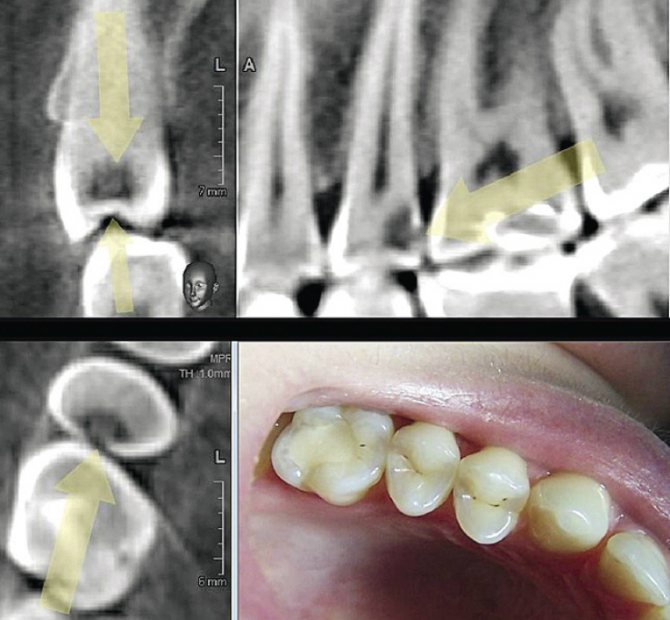
This is due to the fact that in contact caries the area of destroyed enamel is often small, in contact with an adjacent tooth or below the equator, and therefore the defect remains covered by enamel preserved on the occlusal, vestibular and oral surfaces of the tooth (Fig. 1).
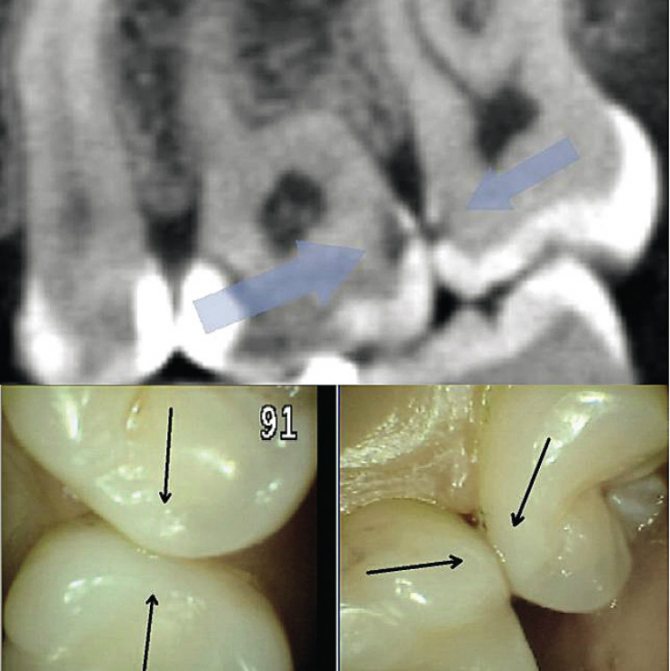
Rice. 1. When examining the contact point of teeth 26, 27 (lower fragment), caries is not visually detected; on the sagittal reformatted computed tomogram in the area of the surfaces of the same teeth proximal to the contact point, demineralization is obvious.
There are many methods for diagnosing caries - from a simple examination of the oral cavity to the use of ultra-modern laser technology DIAGNOcam (Fig. 2).
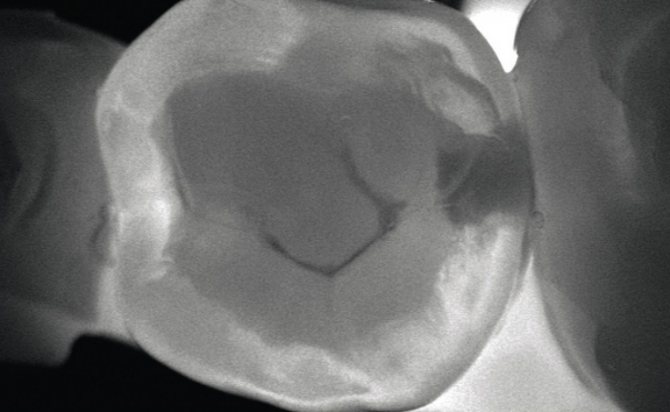
Rice. 2. Saved image of the transilluminated tooth obtained during examination with the KaVo DIAGNOcam.
To diagnose contact caries all over the world, the radiation method is traditionally used. For the first time, a method for detecting proximal caries using X-rays was proposed in 1920 by Raper. The technique was called by the author “bite wing,” which means “bite the wing.” The name is associated with the peculiarity of the shooting and is still used in foreign literature.
To conduct such a study, a film intended for intraoral examination was wrapped with a strip of thick paper and placed in the oral cavity so that the patient, closing his teeth, bit the edges of the strip. Later, to conduct this research, they began to produce a special film in a case equipped with a “wing” - a plane for biting (Fig. 3).
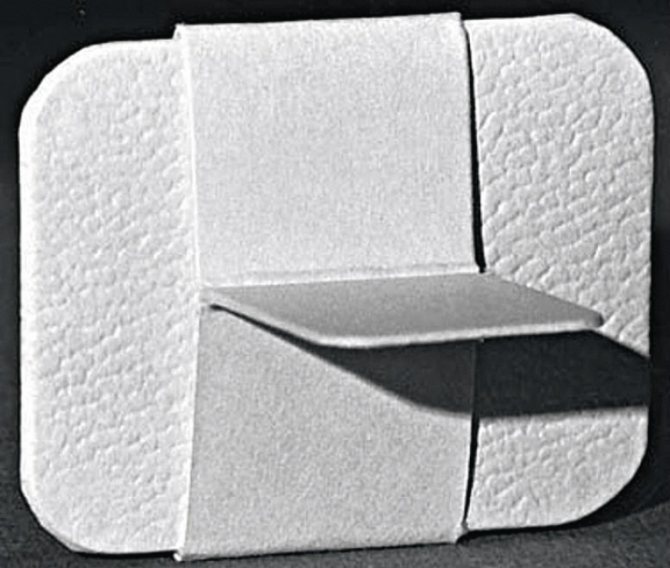
Rice. 3. Film in a special case for shooting using the bitewing technique (reproduction from SC White, MJ Pharoah, Oral Radiology Principles and Interpretation, 2012).
The bitewing technique has been repeatedly described in various publications; in the Russian interpretation, it is traditionally called interproximal radiography. However, recently, for this type of research, the designation “bite shot” has begun to appear in the domestic literature. This incorrect name appeared as a result of the free interpretation of translations of foreign articles without correlation with domestic terminology and historical names.
In Russian-language and foreign literature, a “bite-bite” image (occlusal projection), or more correctly, an occlusal image, is a study in an axial projection with fixation of an 8x8 film in the occlusal plane with the beam directed perpendicularly or at a certain angle to it. The Mac Call&Wald technique was developed in 1957 and is used to examine the condition of the floor of the mouth, hard palate, or as a method of choice for difficulty opening the mouth. Interproximal is a study intended to assess the condition of the proximal (relative to the contact point) surfaces of the tooth and bone tissue of the interroot space.
This type of study includes intraoral radiography performed using the bitewing technique (Fig. 4) and separate intraoral radiography of the tooth in an orthogonal projection.
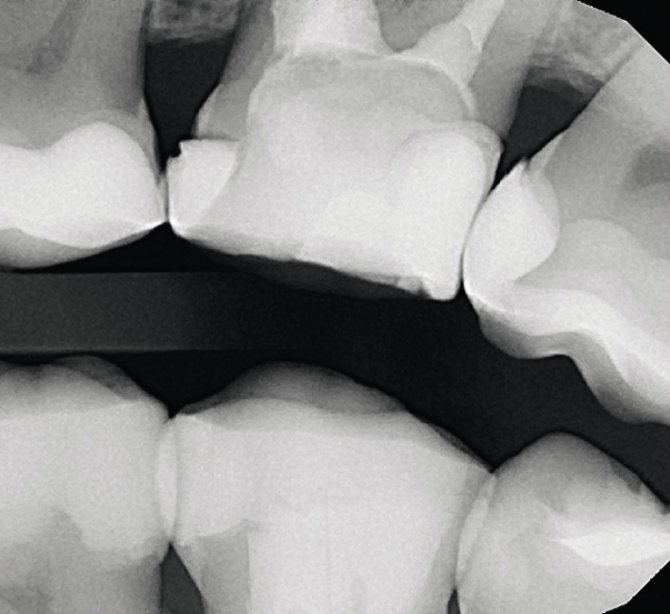
Rice. 4. Interproximal image made using the bitewing technique, examining the condition of the contact points of the maxillary molars.
A feature of interproximal imaging is, firstly, that the image receiver is placed in the oral cavity strictly parallel to the vertical axis and the mesiodistal plane of the teeth being examined. Secondly, the centering of the beam (the direction of the central beam of the beam) is carried out either on the line of closure of the teeth (bitewing, Fig. 5), or in a direct projection onto the interdental space strictly at right angles to the vertical axis of the tooth and the image receiver, that is, orthogonally.
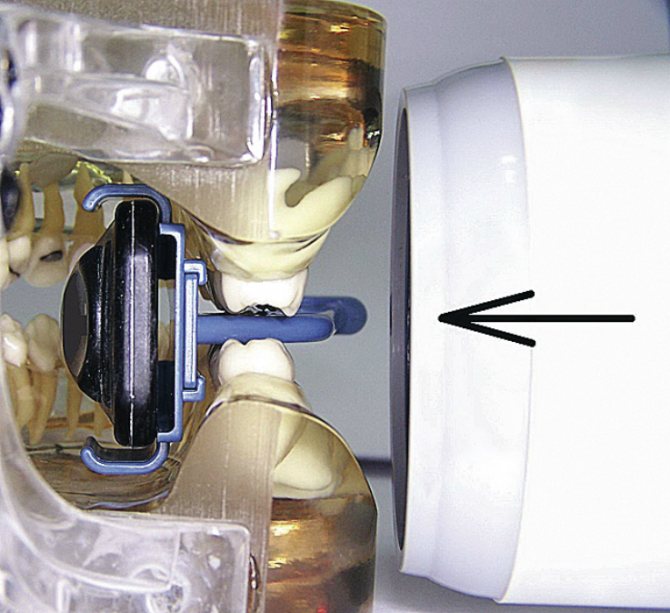
Rice. 5. Demonstration of the position of the positioner in the oral cavity and the direction of the beam during bitewing photography.
The images taken using the bitewing technique show the crowns of the studied teeth in both the upper and lower jaws, the cervical areas, the coronal third of the root and the upper part of the bone tissue of the interdental and interradicular septum. The technique is intended for studying the teeth of the chewing group and is not applicable in the anterior region. With orthogonal photography, the teeth of only one jaw are examined, but in all sections. Examination of teeth in orthogonal projection is only possible with the use of positioning devices. The first such positioner was proposed by Hauberisser back in the 20s of the twentieth century and could easily be made of wire and cork (Fig. 6).
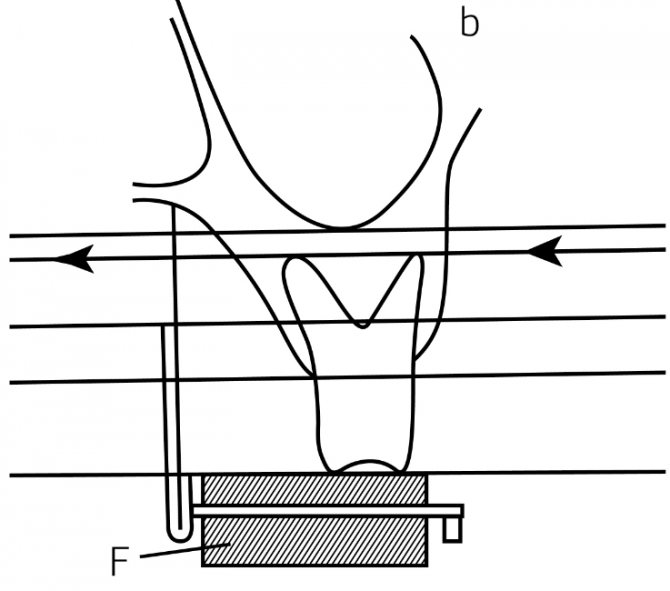
Rice. 6. Hauberisser device, reproduction of the circuit from 1939.
Currently, devices for intraoral film fixation are produced industrially from plastic. Radiography of teeth in an orthogonal projection using a positioner with a guide plane is now often called the parallel method, which is not entirely correct. The term appeared in the 60s and did not indicate that the film was parallel to the tooth, but that the shooting was carried out from a distant focal length.
This reduces beam divergence in the central region and allows for more parallel passage of the central beams, which reduces projection distortion. However, the ray tubes (“dentographs”) used in dentistry at that time had neither a tube nor a collimator and were equipped with only a guide cone, so the term “ parallel shooting."
Currently produced X-ray generators have a tube of a certain length, sufficient to achieve the required parallelism of the beams of rays, so now any type of shooting is carried out with a “parallel beam beam”, and only the positioning method and projection matter. Orthogonal photography is intended not only to study the contact surfaces of the coronal part of the tooth, but also mainly to assess the condition of the periodontium (periodontal tissue). A series of photographs showing all the teeth present in the oral cavity in an orthogonal projection is called “occlusal status” (or full-mouth set of radiographs), and currently this method of radiovisualization is considered optimal for periodontology.
Unlike panoramic photographs (orthopantomograms), where interdental septa are removed in most cases diagonally, which excludes the possibility of adequate diagnostics in periodontology, with orthogonal filming, objects are displayed in a direct (orthoradial) projection at each point of the alveolar part of the jaw. This provides high information content not only in the diagnosis of caries and periodontal diseases, but also in assessing the quality of contact point restorations.
However, due to the limited vertical area to be captured, associated with the specific position of the film in the mouth, there is a high risk of “cutting off the root tips” of the teeth under study, and there is also no possibility of obtaining oblique (eccentric) projections used in endodontics. Therefore, for examination of periapical tissues, an isometric projection is recommended (periapical imaging according to the angle bisector rule, Cieszynski method; for more details, see: Rogatskin D.V., Ginali N.V., “The Art of Dental Radiography,” 2007).
The development of digital technologies ensured the emergence of radiovisiographs, which significantly simplified the conduct of radiation examinations and increased the information content of images. To carry out the study of proximal surfaces and periodontium using a visiograph, a number of special positioners are produced (Fig. 7), the use of which is necessary for these types of surveys.

Rice. 7. Modern Gendex positioner for bitewing shooting.
In addition to positioners, high-quality diagnostics is facilitated by the presence of radiovisiograph sensors of increased area. For example, the widely used radio imaging system Gendex GXS-700 comes with sensors of two sizes: standard - 27x35 mm and enlarged - 31x42 mm. The latter is best suited for the interproximal bitewing technique.
In the last decade, interest in three-dimensional radiodiagnostics, represented in dentistry by cone beam computed tomography (CBCT), has noticeably increased among researchers and practitioners. This type of radiation examination today is undoubtedly the most reliable, objective and informative.
One three-dimensional examination of the maxillofacial area immediately eliminates the need for all other two-dimensional diagnostic studies, since CBCT alone provides complete visualization of each tooth in any projection angle, and also allows for panoramic and volumetric reconstruction of the dentition without projection distortion (Fig. 8).
Rice. 8. Three-dimensional visualization of the carious process on the distal surface of tooth 15.
Due to the absence of the effect of summation of the structures through which the beam passes during a conventional radiation study, tiny foci of demineralization can be detected on a computed tomogram, undetectable using an intraoral camera and not visualized on interproximal images (Fig. 1).
However, despite such high accuracy and information content, when applied to the diagnosis of proximal caries, computed tomography has certain disadvantages associated with the scanning feature. Since during a three-dimensional study the emitter describes a full circle around each point located in the scanning area, the beam is reflected from each hyperdense inclusion at 360°, which ensures the formation of a zone of increased contrast around each foreign inclusion, spreading in the axial plane. As a result, a “dark zone” is formed around each filling and in contact with the artificial crown, visually perceived as a defect in hard tissues (Fig. 9).
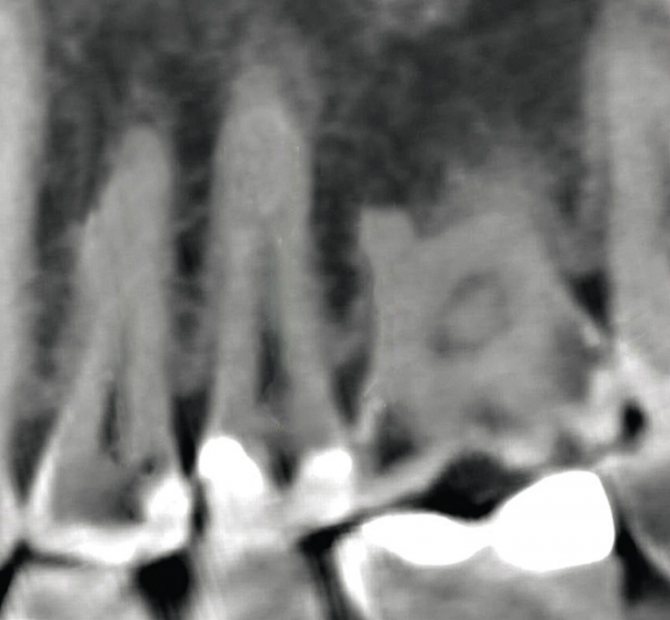
Rice. 9. Sagittal reformation of the area of premolars and molars.
Moreover, if an intact tooth is located between two restorations, then it falls into the zone of an artifact called a “filling defect” and looks like it is affected by caries on both sides (for more details, see: Rogatskin D.V., “Cone-beam computed tomography. Basics of visualization", 2010). In this regard, the diagnostic value of CT in the diagnosis of proximal caries seems somewhat ambivalent. On the one hand, the highest sensitivity and accuracy are obvious when examining teeth that have not been treated and are not in contact with restorations; on the other hand, there is a complete lack of reliability in contact with artificial structures. Thus, it is not possible to reliably diagnose caries that continues under a filling and caries in contact with an artificial crown or filling using CT.
Considering that panoramic zonography (orthopantomogram) gives only a general idea of the condition of the dentition, periapical photographs cannot be used for diagnostics in periodontology and for the diagnosis of contact points, and orthogonal imaging, on the contrary, does not always provide sufficient visualization of periapical tissues and the root canal system , computed tomography should be considered the optimal diagnostic tool in dentistry today. As an additional method, if it is necessary to examine the tooth surface in contact with a high-density artificial structure, interproximal radiography, performed using bitwing or orthogonal techniques, should be recommended.
Classification according to the severity of the process
Clinical observations have established that the severity and speed of development of the carious process determine the methods and tactics of its treatment. Based on the results of these studies, the well-known specialist in the field of dentistry T.V. Vinogradova proposed a classification of caries according to the severity and prevalence of the carious process:
Compensated form of caries
With this form of caries, the average intensity of pathological processes is less than the average intensity for this age group. The disease spreads slowly, carious cavities are lined with hard, pigmented dentin (chronic caries).
Generalized caries
The average intensity of caries approximately corresponds to the average for a certain age group.
Decompensated form of caries
The intensity in the decompensated form significantly exceeds the average for the age groups studied. In this form, the carious process proceeds very intensively; in this form of caries, a large number of carious cavities filled with soft dentin are observed. The extreme form of acute caries is the so-called “systemic damage” of teeth by caries, in which carious lesions are observed in almost all or all teeth in the cervical area.
X-ray diagnostics
Pulpitis is a study using x-rays passing through the tooth tissue and appearing as a picture on the image.
Displayed as dark and light areas. Classic X-rays are gradually fading into the background. Today, specialized devices are used - visiographs, which project images onto a computer screen.
In fact, x-ray is an additional method for diagnosing pulpitis, since with the help of such a study it is impossible to identify pathology. Based on the results, indirect diagnostics is carried out to determine the depth of the carious lesion.
An exception is the purulent form of pulpitis, which leads to the death of the bone structure and pathological changes. This can be seen clearly in the photographs.
For this reason, x-rays should be considered as an accompanying examination method. A physical examination and EDI (electroodontodiagnosis) are mandatory to assess the condition of the pulp.
Classification of caries by localization
Scientist Black (USA) developed a classification of carious cavities by location:
- Class I: damage to cavities in the area of fissures and natural recesses of the teeth;
- Class II: damage to cavities located on the contact surfaces of small and large molars;
- Class III: damage to cavities located on the contact surfaces of the incisors and canines without involving the cutting edge;
- Class IV: damage to cavities located on the contact surfaces of the incisors and canines, involving the cutting edge and corners;
- Class V: damage to cavities located in the neck area of all groups of teeth;
- Class VI: damage to cavities of atypical localization - the cutting edges of the frontal teeth and the cusps of the chewing teeth.
Four stages of development
Pathology goes through several successive stages. At first, this is a small contrasting spot that does not affect deep formations and does not lead to complications with timely treatment. What caries looks like between teeth at different stages of its spread:
- Elementary. Only the upper enamel layer thins. Small white or dark spots are found where surfaces touch.
- Surface. The enamel begins to deteriorate, forming depressions that can be felt by running your tongue over them. Darkening is clearly visible in the interdental space.
- Average. Blackened areas are visible to the naked eye. Symptoms appear, such as sensitivity to cold, hot and sour, and bad breath.
- Deep defeat. The diseased crown begins to collapse. The spaces between adjacent incisors, canines or molars widen. The patient feels severe paroxysmal pain, sometimes there is bleeding after biting food, and the mouth smells rotten. Teeth may become partially chipped or fall out completely.
Symptoms
It is quite difficult to detect the disease in its earliest stages. The first unpleasant signs appear when the integrity of the enamel is damaged. A person begins to react to temperature stimuli, especially food and drink. It is not so easy to examine a carious cavity, since the inner surface of the units may be damaged.
Characteristic symptoms that indicate a problem and require urgent contact with a dentist:
- painful reaction to hot, cold, sour, sweet;
- increased sensitivity when performing routine hygiene procedures;
- foul breath associated with the proliferation of pathogenic bacteria and decay of plaque (experts have not proven whether there can be caries between teeth that are regularly cleaned of particles of eaten food with an irrigator);
- the appearance of white or dark spots on the enamel;
- paroxysmal pain (the larger the damaged area, the more intense the pain);
- the presence of visible carious cavities that can be felt with the tongue (in advanced situations).
It is better not to bring the disease to such an extent that severe pain appears and black spots are visible to the naked eye. With periodic preventive checkups at the dentist, the problem can be identified at the earliest stages.