Today, many modern diagnostic methods are used in dental practice, but classical X-ray examination still remains the leading method of additional examination of the maxillofacial area. In therapeutic dentistry, radiography is used to diagnose periodontal and periodontal pathologies, in orthopedics - to draw up a treatment regimen depending on the condition of the remaining teeth. In surgical practice, radiography is used to identify injuries, cysts and tumors. There are several techniques for X-ray examination of the maxillofacial area, one of which is intraoral radiography.
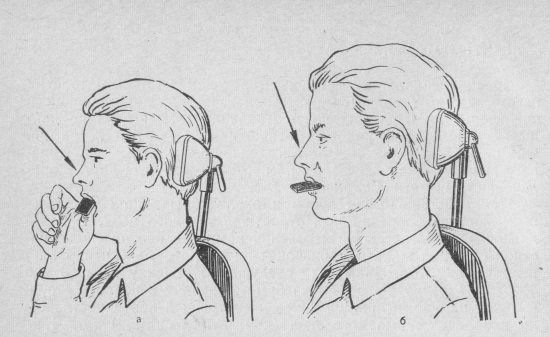
Position of the patient during intraoral dental photographs
Intraoral x-ray examination is carried out using modern x-ray machines, portable or portable, which allow you to obtain images on a special x-ray film. This method of radiodiagnosis is the main way to study the condition of the teeth and bone tissue of the upper and lower jaw. There are several methods for performing intraoral x-ray examination:
- Contact intraoral radiography.
- Occlusal radiography (bite radiography).
- Interproximal radiography.
Intraoral systems and their capabilities
Intraoral systems consist of a small optical sensor with a video camera, a computer and associated software. During operation, light is projected onto the required areas in the oral cavity, sensors receive it after reflection from tissues and, based on the data received, the computer creates a three-dimensional model. It completely replaces the usual casts, and with very high accuracy. Moreover, there is a fundamental possibility of connecting this system both to a 3D printer and directly to dental equipment. Modern representatives of such scanners are able to recognize the color of teeth and even the presence of caries.
Advantages of a computer or digital 3D impression
So what are the benefits of intraoral systems?
- Comfort and speed of the procedure, especially for patients with an increased gag reflex. There is no impression material or large impression trays in the mouth; the process itself takes a few minutes.
- The patient can see the resulting 3D models on the monitor. They are realistic, the scanner distinguishes not only the colors themselves, but also plaque on the teeth, as well as soft tissues of the oral cavity.
- The quality of the impression can be assessed immediately and in case of any defect, only this area can be rescanned, and not the entire jaw.
- The accuracy of the resulting models is measured in nanometers. This eliminates errors in data acquisition due to, for example, irregularities during the preparation of the impression material, ingress of blood or saliva, the presence of air bubbles, etc. This makes it possible to take into account the smallest individual characteristics of the patient and create the most accurate aesthetic restorations.
- The process of transferring data to the dental laboratory is significantly accelerated, and there is no risk of deformation of the impression and transmission of infection with it.
- The process itself is simple, does not require lengthy special training and is economical, because there is no need to use consumables.
- Treatment time and working time costs are reduced, since additional visits to the doctor to take clarifying impressions become unnecessary, especially in the case of the installation of extended structures; no need to make individual spoons; the same 3D impression can be sent to multiple locations or used for multiple purposes.
- The clothing of the medical staff cannot become dirty with impression materials.
Disadvantages of 3D impressions
Digital impression of teeth on a computer screen The disadvantages of these systems include the difficulty of recognizing hard-to-see places. The edges of the prosthesis may be obscured if the examination is performed against the background of bleeding in the patient.
It is obvious that with so many advantages, intraoral scanning will gradually replace classical technology. Currently, this is hampered by the conservatism inherent in medicine and the high cost of equipment. However, there is a large variety of systems from different manufacturers on the market. Among them, one of the best is the TRIOS TM scanner from 3Shape.
Occlusal radiography
Contact x-ray examination of bite, or occlusal x-ray, got its name because the picture is taken with the teeth closed, between which the sensor of the device is located. This type of diagnosis allows you to visualize a section of the alveolar process in the area of 4–5 desired teeth, where large pathological formations, impacted teeth, and stones in the salivary glands are clearly visible. Using this method, it is possible to assess the condition of the tissues of the hard palate and floor of the mouth, and identify the location and extent of the fracture. Occlusal radiography is often used in the examination of children and adolescents, as well as patients with limited mouth opening and a pronounced gag reflex.
Intraoral scanner TRIOS TM
This model has all the advantages of intraoral systems. This thin flexible device penetrates even hard-to-reach areas of the oral cavity without causing any discomfort and does not require the use of anti-reflective powder. The color images obtained with its help are highly accurate even at the boundaries of the restoration.
The complex process of modeling an impression of various parts of the jaw now takes only a few minutes, since the scanner computer is connected to the milling department of the dental workshop.
Petrikas pulpectomy / Chapter 05 Radiography / 04 Intraoral radiography. Ways. Goals
Intraoral radiography. Ways. Goals
There are four main intraoral methods for examining teeth:
1) interproximal or in a bite cassette, bite-wing (Fig. 5-16),
2) parallel or rectangular, or long-focus (Fig. 5-17),
3) isometric or bisector, or Cieszynski method (Fig. 5-18),
4) occlusal technique (Fig. 5-7.3) is performed with a large film (at least 5.7 × 7.6 cm) and solves special, usually non-endodontic problems, and is therefore rarely used.
Rice.
5-16.
Scheme of intraoral interproximal radiography (bite-wing). The central beam is directed perpendicular to the film and the axis of the tooth. The film is located parallel to the tooth axis [128].
Rice.
5-17.
Scheme of performing intraoral apical radiography in a parallel way. The axis of the tooth and the film are parallel, and the central ray is perpendicular to them [128].
Rice.
5-18.
Scheme of performing intraoral apical radiography using the isometric method along the bisector of the angle (according to Cieszynski). In addition to the spatial distortion of the image of the upper molar, the zygomatic process and zygomatic bone are superimposed on its apical region [128].
AND
Interproximal and parallel methods provide a minimum of distortion, since the central beam is directed perpendicular to the long axis of the tooth and the film. The first (bite-wing) is used mainly for lateral teeth and is highly sensitive in diagnosing contact caries and the condition of marginal periodontium.
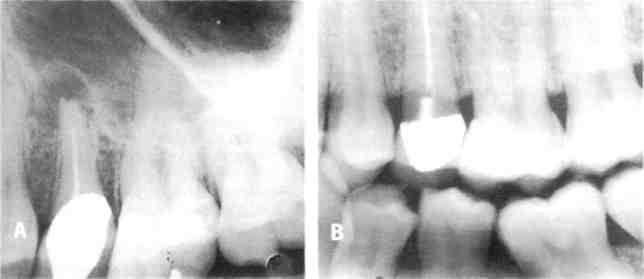
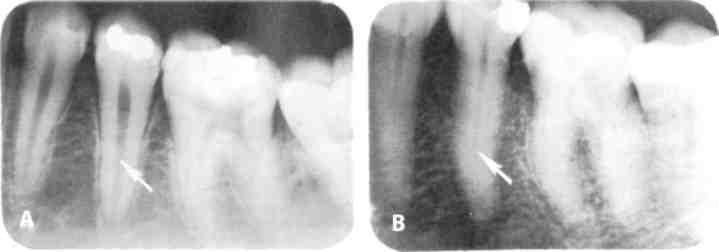
Rice.
5-19.
Radiography of the lateral part of the upper jaw in different ways in the same patient. A - A radiograph taken along the bisector of the same area reveals extensive rarefaction in the periapical region of the upper second premolar. B, Interproximal (bite-wing) radiograph shows a large cavity under the artificial crown, which is not visible on the bisector image. [154].
ABOUT
An overview of the dentition can be obtained with only 3-4 photographs. The fact that the apexes of the roots are not included in the image precludes its use for endodontics (Fig. 5-19). Widely used in adolescence, until the patient has endodontic problems.
Rice. 5-20. Images of objects and teeth using bisector (top) and parallel (bottom) techniques
“Apical” are the second and third methods, competing with each other and claiming to be universal. Currently, the traditional isometric or bisector method is being replaced by a parallel one, due to the high accuracy of the latter175 (Fig. 5-19 and 5-20). Its vertical distortion is no more than 3%, which allows, for example, when determining the working length of a tooth to be limited to a diagnostic radiograph. A special film holder oriented to the tube - a positioner (Fig. 5-3 and 5-17) ensures precision and a high degree of repeatability (standardization) of the image. The latter is very important when assessing the effectiveness of treatment in the long term95. The parallel technique cannot be performed without a film holder or positioner. Using a parallel technique, it is possible to bypass the zygomatic bone and better navigate the state of the periapical tissues (Figs. 5-17 and 5-19). Parallel and interproximal images can only be performed on modern X-ray machines with a long tube (Table 5-1).
Table
5-2.
Advantages and disadvantages of photo and digital radiography
| Chemical radiography | Digital radiography | |
| X-ray machine | Any | Modern |
| Exposition | Big | Minimum |
| Sensor | Disposable film | Reusable sensor |
| Materials | Constantly expendable | Low consumption |
| Assistant | Required | No |
| Duration | Significant | Seconds |
| Additional room | Often necessary | No |
| Image processing | No | Electronic |
| Image quality | High, but depending on many subjective factors | Satisfactory, progressive |
Rice.
5-21.
Distortions of the position of the roots and tubercles of the teeth during radiography along the bisector of the angle: NK - palatal root, SB - buccal root, NB - palatal tubercle, SB - buccal tubercle, SB - zygomatic process.
Rice.
5-22. A series of endodontic radiographs - diagnostic (A), final control (B) and control after 5 years (C).
A
— a root cyst from the central lower incisor is diagnosed, which led to tooth displacement;
B — during filling of the main canal, additional canals are sealed;
C—complete restoration of bone and periodontium [223].
Distortion in traditional apical radiography is associated with the direction of the central ray at different angles to the axis of the tooth and the film (Fig. 5-21). These distortions are located vertically: the length of the tooth, the position of the apexes of the roots and masticatory cusps. To correctly read the anatomy of a tooth, the doctor must navigate the logic of these distortions (Fig. 5-18). On the lower jaw, especially in the area of the molars, these distortions are less pronounced. Using the bisector of the angle between the film and the axis of the tooth as a guide for directing the beam (Cieszynski’s rule - 1907) requires a certain vertical position of the apparatus head: at a positive angle for the upper teeth and at a negative angle for the lower ones. The projections of the apexes of the roots for the upper teeth lie along the line from the tragus of the ear to the base of the nose, for the lower ones - along the edge of the lower jaw, just above it (Table 5-3).
Table
5-3.
The vertical inclination angle of the head of the X-ray machine for different teeth in degrees using the traditional bisector method.
| Plot | Jaw | |
| Upper | Lower | |
| Incisors | +55-60° | -20° |
| Fangs | +45° | -15° |
| Premolars | +35° | -10° |
| Molars | +0-25° | -5° |
With the parallel technique, the right angle between the central beam and the film is ensured by the film holder and the X-ray tube locator - positioner. However, you should maintain a right angle with the tooth being removed, since, for example, the front teeth are not vertical. An error of 10° is acceptable.
Depending on the purpose, apical radiographs can be of four types: diagnostic, working, final control and control in the long term after treatment
(Fig. 5-22, 5-23).
Rice.
5-23.
A series of endodontic radiographs - diagnostic (A), final control (B) and control after 2 years (C): A - apical periodontitis of the first lower molar with damage to the periapical areas of both roots and bifurcation; B - immediately after filling; C - complete restoration of the periodontium, including bifurcation, new carious cavities (arrows), the stage of the unclosed apex of the first premolar. [175]
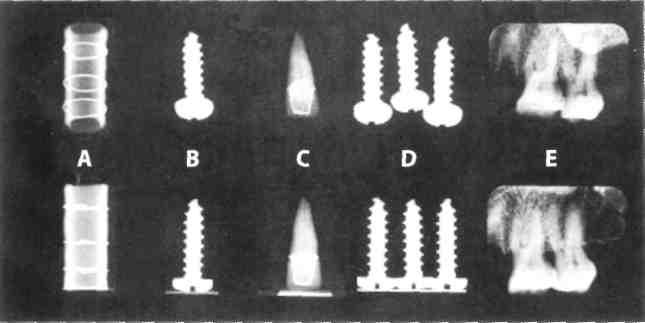
The diagnostic role of radiography is to detect hidden carious cavities on the contact surfaces of the lateral teeth, recurrent caries, in the assessment of restorations, previous treatment, pulpal dentin resorptions (Fig. for problem 5, Chapter 8, Fig. 4-8, 2-15, 2- 21) in identifying denticles (Fig. 5-24), which are common (15% of teeth). It is necessary to analyze the anatomy of the tooth: the pulp chamber (Fig. 10-11), the number of roots and canals. This applies more to operational operational issues. Therefore, a diagnostic image is often called preoperative. Evaluation of the canal comes down to determining its longitudinal shape (straight, curved) and diameter (Fig. 5-25). The canal can be wide or narrow, sclerotic. Important points are the level of the end of the canal, whether the apical foramen is determined or not, the presence of additional canals, etc.
Rice.
5-24.
X-ray detectable denticles (arrows) in the tooth cavity [239].
Rice.
5-25.
The size of the tooth cavity in a young (A) and elderly (B) patient on a radiograph of the second lower premolar. The arrow shows the wide (A) and narrow (B) channel [239].
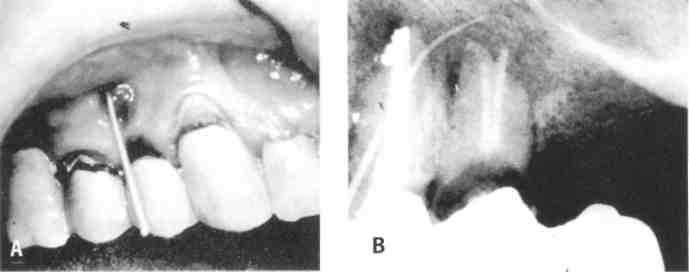
Rice.
5-26.
Definitions of the route of the fistula tract.
A - fistula located between two premolars, into which a gutta-percha pin is inserted,
B - the pin selects the second premolar [257].
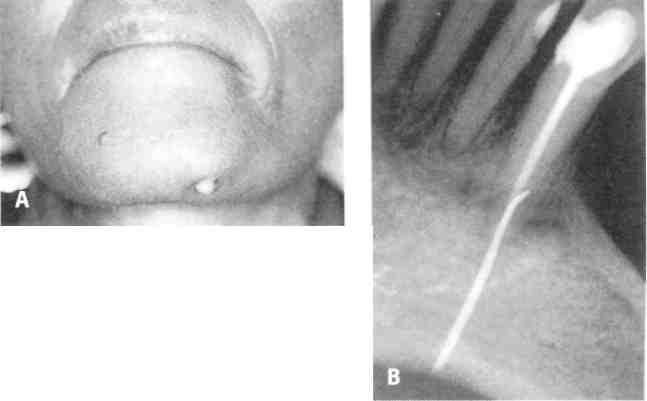
Rice.
5-27.
A - Extraoral fistula on the skin of the chin.
B-The fistula route was traced using a gutta-percha point to a mandibular canine that was treated endodontically. [177]
During diagnosis, special techniques can be used, for example, examining the route of the fistula tract using a gutta-percha pin (Fig. 5-26) or determining the depth of the pathological gingival pocket using a silver pin. One of the main tasks of X-ray diagnostics is to assess the condition of invisible periapical tissues.
Control X-rays also play an important diagnostic role, since in Russia periapical pathology is most often observed in endodontically treated teeth. The ratio of primary and secondary (needing retreatment) apical periodontitis is 1:3 according to our epidemiological studies79. Therefore, each pulpless tooth needs an x-ray assessment when you next visit the dentist.
Indications
Intraoral scanners can be used for almost any dental damage. They are used to study the dental system in cases where aesthetic prosthetics are planned. Specially conducted studies have shown a very high agreement between scanning results using these devices compared to laboratory scanners. Where a lot of work is done with individual abutments, metal-free ceramics and extended structures supported by implants, the use of these systems is economically and professionally feasible, even despite their high cost.
Indications for use
Dental radiography is used for two main purposes: to diagnose and evaluate the quality of treatment performed.
Allows you to detect the following diseases:
- hidden carious lesion;
- pulpitis (inflammation of the neurovascular bundle of the tooth);
- cyst at the roots of the teeth;
- periodontitis (purulent inflammation of the tissue between the root of the tooth and the hole in which it is located);
- gum disease, in which bone tissue atrophies (periodontitis, periodontal disease);
- neoplasm.
Intraoral radiography also helps evaluate the results of procedures such as:
- root canal filling;
- treatment of periodontal diseases.
Features of radiography using special techniques
- Enlarged panoramic radiographs in direct projection
allow us to evaluate the frontal parts of the jaws. The anode of the tube is inserted into the oral cavity, the cassette is pressed against one of the jaws. The image is enlarged by one and a half times. - An orthopantomogram
is a detailed image of the jaws. The tube and film/intensifying screen cassette trace a partial circle around the patient's stationary head. At the same time, the cassette simultaneously rotates around its axis vertically. - A teleradiogram
is performed at a long focal length. The volume being examined and the cassette are moved away from the tube by 1.5-2, and sometimes 3-4 m. This allows for a greater degree of enlargement of the bone area. - Radiovisiography, or computer digital radiography.
The radiovisiograph consists of a PC, monitor, keyboard, mouse, sensor, information processing board, printer and software. The picture is taken on the sensor and transferred to the monitor for further processing. The radiation exposure of the sensor is 4-9 times less than with a conventional image. The method allows you to quickly obtain digital images, which are much larger than on an intraoral radiograph, while the bone tissue is well visualized.