Goiter of the thyroid gland is not quite the correct name; doctors use either the term goiter or enlargement of the thyroid gland. A goiter in humans is not at all the normal anatomical formation in the esophagus that all birds have; a goiter is a pathology of the thyroid gland.
- What is a goiter?
- Causes of goiter
- Classification of thyroid diseases
- Diagnosis of thyroid goiter
- The first signs and symptoms of thyroid goiter
- Treatment methods
- Complications
- Goiter prevention
What is a goiter?
In medicine, goiter refers to all benign neoplasms in the thyroid gland, both detectable by touch and already visible. A goiter is a knot in the thickness of unchanged tissue or an increase in the entire volume of the gland. With nodules it will be nodular or multinodular , and simply an increase - diffuse and a mixture of them in the form of a diffuse-nodular goiter .
On average, a diffuse version of goiter is found in every third person, but in different regions of Russia, benign lesions of the gland of various types - nodes or enlargement are found in 5% - 70% of residents, and the vast majority are women. It is not known why women are more susceptible to the disease; a direct connection between the level of production of thyroid hormones and the activity of the reproductive organs has been identified, and the leading cause of goiter is also explainable.
Causes of goiter
Due to the disease, goiter can be sporadic and endemic, and in this classification they focus not on the individual development of the pathology, but on the state of goiter morbidity in the region as a whole. The pathology is endemic in areas where goiter of any size and shape is found in every twentieth child and every third adult.
The most common causative factor in the development of pathology is iodine deficiency, which leads to a decrease in the production of iodolipols by thyroid cells, for which the production of glandular tissue growth stimulants increases compensatoryly. The enlarged glandular tissue is actually a goiter, which over time undergoes involution with the formation of nodules.
The formation of goiter is helped by a defect in the synthesis of thyroid hormones or perverted sensitivity of cells to them, taking certain medications that promote goiter growth and are called “goitrogens”. Goitrogens or thyreostatics are used to treat thyrotoxicosis. Pathology can be caused by some components of food; all of them have the ability to block the production of thyroid hormones; it is believed that soy flavonoids and thiocyanates contained in a variety of cabbages, corn and tobacco leaves have a particularly active effect on glandular tissue.
Hereditary predisposition is also important for the development of the pathological process, but specific genes have not yet been identified.
Book a consultation 24 hours a day
+7+7+78
Classification of thyroid diseases
All processes in glandular tissue are divided:
- inflammatory - thyroiditis;
- autoimmune thyroiditis too;
- benign, including those filled with secretions - colloidal or nodules of glandular cells - adenomatous;
- malignant - cancer of various cellular variants, the most favorable are papillary and follicular, aggressive - medullary, as well as poorly differentiated and its “extreme” type - anaplastic.
According to the dysfunction, and the thyroid gland has one function - the production of hormones, goiter variants are distinguished:
- non-toxic, which is also referred to in the literature as euthyroid, when the production of thyroid hormones does not change;
- toxic occurs in two clinical variants: thyrotoxic occurs with hyperfunction of the thyroid gland and the pathological condition caused by this is called thyrotoxicosis;
- a decrease in endocrine production is characteristic of myxedema, and the condition caused by a lack of thyroid hormones is called hypothyroidism.
To determine the tactics for managing a patient with thyroid pathology, the Bethesda cytological classification is used with six categories, from “category 1” meaning uninformative analysis, benign formation - 2, through atypia and neoplasia, suspicion of cancer and cancer itself - starting from “3” categories".
Thyroid diseases
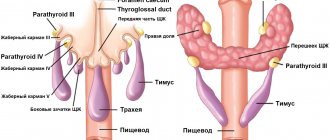
ACCORDING TO WORLD STATISTICS, THYROID DISEASES ARE FOUND IN ALMOST 30% OF THE PLANET'S POPULATION. AMONG WHICH THE MOST COMMON DIFFUSE GOITER (MAINLY IN REGIONS WITH IODINE DEFICIENCY), NODULES, ALSO CURRENTLY THERE IS AN INCREASE IN AUTOIMMUNE PATHOLOGY OF THE THYROID GLAND. The global nature and importance of this problem made it possible in 2009. Experts from the European Thyroid Association propose to celebrate World Thyroid Day on May 25. This initiative was supported by all other medical societies dealing with thyroid pathology: American, Latin American and Asian. World Thyroid Day has five main goals: 1. raising public awareness about the problems associated with thyroid pathology and their medical and social significance; 2. raising awareness about the prevalence of thyroid diseases and methods for their early detection; 3. promotion of prevention programs and educational programs in the field of thyroid pathology; 4. promotion of modern methods of treating thyroid diseases; 5. increasing the availability of medical care in the field of thyroid diseases. Currently, the Republic of Belarus has built a clear system of providing care to patients with thyroid pathology. According to the Decree of the Ministry of Health of the Republic of Belarus dated August 12, 2021 No. 96 “On approval of the Instructions on the procedure for medical examination,” the detection of thyroid pathology is carried out at an outpatient appointment by pediatricians and general practitioners. If there are dysfunctions of the thyroid gland, patients are referred to an endocrinologist who provides medical care in accordance with the order of the Ministry of Health of the Republic of Belarus dated July 2, 2013 No. 764 “Clinical protocols for the diagnosis and treatment of the adult population with diseases of the endocrine system when providing medical care on an outpatient basis.” In 2021, it is planned to rework clinical protocols in order to optimize diagnostic and therapeutic approaches for diseases of the endocrine system, including thyroid pathology. Since the beginning of 2000, the republic has been actively working to eliminate iodine deficiency using the most effective method of mass prevention - the use of iodized salt. Currently, the Republic of Belarus has established production and ensured the availability of iodized salt, which allows the population to receive a sufficient amount of iodine and, accordingly, prevent its deficiency. The results of the implementation of the strategy for eliminating iodine deficiency in the Republic of Belarus allowed the International Committee for the Control of Iodine Deficiency Diseases and the Global Iodine Network to include Belarus in the list of countries that have achieved target levels of iodine nutrition. The measures taken to eliminate iodine deficiency led to a decrease in the primary incidence of nodular goiter (97.5% in 2000; 88.14% in 2021) and a more than 5-fold reduction in the primary incidence of endemic goiter (from 318.9% in 2000 to 59 .09% in 2021). In the Republic of Belarus, over the past five years, there has been a clear decrease in the primary incidence rate and the total number of children with thyroid dysfunction due to the active implementation of the state program of mass iodine prophylaxis. In the structure of thyroid diseases in children, simple non-toxic goiter predominates. At the beginning of 2021, 13,636 patients under the age of 18 were observed with this diagnosis. One of the important criteria for the adequacy of iodine supply to the child population of the republic is the incidence rate of congenital hypothyroidism. Primary screening is performed in all obstetric institutions of the Republic of Belarus. The results of screening for primary congenital hypothyroidism indicate a level achieved that is adequate to the European average: in 2014, 1 case of hypothyroidism was identified per 4,216 newborns. At the same time, over the past 15 years there has been an increase in autoimmune pathology of the thyroid gland. Thus, the number of patients with primary hypothyroidism increased 8 times (in 2000 - 11,078 people, in 2015 - 87,446 people), which is due not only to the accumulation of patients with this diagnosis, but also to the increased availability and accuracy of laboratory diagnostics. The primary incidence of primary hypothyroidism during this period increased 4.5 times (22.55% in 2000 and 94.94% in 2017). One of the most common causes of hyperfunction of the thyroid gland is Graves' disease (diffuse toxic goiter), which requires careful monitoring and long-term differentiated treatment. The primary incidence of diffuse toxic goiter has almost doubled over 15 years: from 6.21 in 2000 to 11.0 in 2021. In the Republic of Belarus in the last decade there has been an improvement in the diagnostic capabilities of thyroid pathology, both in children and adults. Ultrasound examination of the thyroid gland is carried out in all regions of the republic, and hormonal examination of thyroid status is carried out at the inter-district level. At the regional level, fine-needle aspiration biopsy under ultrasound control and thyroid scintigraphy are performed. The THYROID GLAND is a small organ measuring 2-4 cm. It is located in the anterior part of the lower part of the neck under the thyroid cartilage. It got its name from him. The thyroid gland consists of a right and left lobe, connected by an isthmus. Sometimes a narrow and long pyramidal process extends upward from the isthmus. Like a ring, the gland covers the trachea. Normally, the gland is so small that it cannot be felt during examination. On the posterior surface of the thyroid gland are four small parathyroid glands. They have a separate blood supply system and a separate function from the thyroid gland.
Function.
For many people, the thyroid gland is a mysterious, almost mystical organ. And an organ that is greatly feared. They don’t know it, don’t understand its function – and that’s why they are afraid. Some myths regarding the thyroid gland should be dispelled. The only function of the thyroid gland is to produce hormones. The gland produces and releases three hormones into the blood: - triiodothyronine (thyroxine) or T3; - tetraiodothyronine or T4; - calcitonin. The parathyroid glands produce the fourth parathyroid hormone, or parathyroid hormone. Thyroid hormones influence all metabolic processes in the body. The main direction of their influence is the speed of all processes. With a normal amount of hormones, all physiological processes in the body are balanced and correct. When the level of thyroid hormones is low, all processes slow down. With increased hormone levels, metabolism accelerates. A decrease in thyroid hormone levels is called hypothyroidism, and an increase is called hyperthyroidism. Thyroid hormone levels cause the opposite conditions. There are also common manifestations of hypothyroidism and hyperthyroidism caused by hormonal disorders: - fragility, dryness and hair loss, brittle nails; - general weakening and exhaustion of the body; — calcium metabolism disorders with the development of osteoporosis in the bones; — menstrual irregularities in women and associated infertility; - a breathing complication caused by compression of the trachea by an enlarged thyroid gland. Disorders of thyroid hormones are especially severe in women and children. Women experience menstrual irregularities due to multiple hormonal disorders. This often ends in infertility, which cannot be treated. In children, an insufficient amount of hormones during development leads to mental retardation (disease - cretinism). Skeletal development slows down and various forms of damage to internal organs occur.
Calcium metabolism.
The third thyroid hormone, calcitonin, regulates calcium metabolism in the body. It acts together with the hormone of the parathyroid glands - parathyroid hormone. And their effect is the opposite. Calcitonin helps increase calcium levels in the blood. Parathyroid hormone leads to a decrease in calcium in the blood. Normal calcium regulation is possible with the combined action of these two hormones. If the level of one of these hormones is absent or decreased, calcium imbalance occurs. Bone destruction often develops - osteoporosis. The most common thyroid disorder is due to iodine deficiency. Iodine is a trace element that a person receives from the environment through food and water. But sometimes the amount of iodine in nature is limited. Then not enough of it enters the human body. With a limited amount of iodine in the body, the thyroid gland cannot synthesize enough hormones. And stimulating commands from the pituitary gland (in the form of increased TSH) enhance the functioning of the thyroid gland. As a result of this stimulation, the size of the thyroid gland increases. More blood passes through a larger volume of the gland and more iodine is captured. An increase in size of the thyroid gland is called a goiter. Such an enlargement of the thyroid gland is observed in almost all people who live in areas poor in iodine. Enlargement of the gland in this case is not a disease, but only an adaptation to environmental conditions. This is an endemic goiter. Hormone levels remain normal. Metabolism is not affected either.
Chernobyl is the “sworn friend” of doctors.
These days, endocrinologists do not complain about the lack of patients with thyroid dysfunction. The “hormone factory” is malfunctioning for many residents of Belarus. However, the increase in incidence is not directly related to the 1986 disaster. The April explosion drew attention to the problems of the organ - the source of thyroxine. After the tragedy, a program of regular screening of the population appeared. The Republican Scientific and Practical Center for Radiation Medicine and Human Ecology was created. Hidden pathologies of the thyroid gland became obvious. Harmless changes no longer “leak through” the “fine sieve” of medical control. This situation is perfectly illustrated by the saying “There was no happiness, but misfortune helped.” Unfortunately, too serious a misfortune. The victims of the terrible cloud were primarily accident liquidators and children under 18 years of age. Against the background of radiation damage, thyroid cancer often developed. The organ, “eaten” by destructive cells, had to be removed. Patients were expected to undergo lifelong replacement therapy - eternal intake of thyroxine. Today, the most common diseases of the vulnerable gland are simple non-toxic goiter, nodular goiter and autoimmune thyroiditis. Diffuse toxic goiter (Graves' disease) also makes itself known. The last two “misfortunes” are the result of an imbalance in the immune system of a weak organism. “Ordinary” enlargement of the thyroid gland is a sad reality of the “atomic” age and a consequence of poor ecology. Currently, 199,228 residents of Belarus are under medical supervision for thyroid diseases. This number is comparable to the prevalence of diabetes mellitus. The fewest visitors to endocrinology offices are in the Minsk region - about 20,000 people. The sad leadership belongs to the Gomel region - 47,600. Thyroiditis accounts for 40,000 diagnoses, simple nodular goiter appears under the skin of 81,000 citizens. Diffuse goiter poisons the existence of 43,000 inhabitants of Sineokaya. By the end of 2009, 9,684 Belarusians had undergone surgical treatment for thyroid cancer. Almost all “core” diseases, with the exception of malignant tumors and diffuse toxic goiter, do not require surgical intervention. Conservative treatment helps to “avoid” the trouble. However, cancer in this case is not a death sentence of merciless fate. This is one of the most “favorable” types of such pathology with a comforting prognosis. After removal of the gland, the body is supported by hormonal drugs.
Beware, invisible aggressor!
An unpleasant property of thyroid diseases is “sneaky” secrecy. Most of them do not distinguish between “bright” symptoms. Patients do not always feel a “tight collar” or an “invisible collar”. Patients may not experience discomfort when swallowing. Voice changes also occur infrequently. The pathogenic process sometimes proceeds unnoticed, gradually eroding the protective forces. The “winners” are people with fragile physiques. On a thin neck it is difficult not to notice a voluminous goiter. Graves' disease does not belong to the "masters of camouflage". It is quite difficult to ignore “enlarged” eyes, tachycardia, short temper, trembling hands, sweating and weight loss while eating high-calorie foods. Mature citizens should be especially vigilant. Women over 35 years of age join the risk group. After overcoming this “numerical threshold,” ladies need to undergo a thyroid examination once a year. A similar procedure is prescribed during pregnancy. It must be said that 85% of cases of diseases of this organ are detected in the fair sex. Don't forget the way to the medical office. However, the predicted slight enlargement of the thyroid gland occurs during adolescence, during gestation and after menopause. Palpation, ultrasound, and determination of thyroid hormones help to establish the diagnosis.
“Companions” of iodized salt.
Including iodine-containing foods in your diet will help protect you from endocrine problems. In addition to “improved” sodium chloride, seafood is rich in it: kelp, shrimp, oysters, squid, mussels, crabs. “Iodine-bearing” fish include flounder, cod, herring, halibut, tuna, salmon, and sea bass. Some “gifts from the garden” are also useful in this regard: eggplant, asparagus, spinach. Tropical sun can be a provocateur of thyroid diseases. You should not “smoke” under the rays of the “vacation” star from morning to night. When at a hot resort, be sure to wear a hat with a wide brim that covers the neck area. Radiation from a computer monitor is also harmful. You can’t work behind a screen “all day long.” From time to time you need to take a break and ventilate the room. It is better not to ignore “banal” infectious diseases. Even a “harmless” ARVI sometimes leads to “unhappy” consequences. Avoid stressful situations whenever possible. The thyroid gland’s best “friends” are a healthy lifestyle and good sleep. As the thyroid gland grows, the size of the organ rapidly increases. But at the same time, growth is accelerated and therefore distorted. The vessels do not have time to form a sufficient blood network in the overgrown tissue of the organ. As a result of this, dense areas with insufficient blood circulation appear in the enlarged organ. In this metastasis, the thyroid tissue thickens. A gland node forms. There may be several such nodes. Typically, the formation of nodes occurs against the background of an increased size of the gland itself - a nodular goiter occurs. Often, atrophy of thyroid tissue occurs inside the node with the formation of a cyst in the gland.
Diffuse toxic goiter.
This is a disease that is caused by a significant increase in the level of thyroid hormones - T3 and T4. Another, more well-known name is Graves' disease. With this disease, pronounced symptoms of hyperthyroidism occur. Endogenous (internal) poisoning of the body with thyroid hormones occurs. Therefore, the disease is called toxic. The reasons are different - mental trauma, autoimmune disorders, inflammation in the thyroid gland and others. But the undeniable fact is that increased production of thyroid hormones by the gland is provoked by disorders of the pituitary gland (or the brain itself). An increase in TSH levels leads to increased thyroid function. An increase in the level of its hormones provokes hyperthyroidism. Manifestations of diffuse toxic goiter. From the cardiovascular system: - tachycardia (rapid heartbeat); - arrhythmia (atrial fibrillation, extrasystole); - arterial hypertension; - increased pulse pressure (the difference between systolic and diastolic pressure); — chronic heart failure with peripheral edema; - ascites - accumulation of fluid in the abdomen caused by heart failure; - anasarca - total swelling of the entire body. From the nervous system: - tremor of the arms, especially those extended in front of you; - increased tendon reflexes; - muscle weakness; - weakness, headache. From the mental side: - increased activity; - anxiety; - anxiety; - insomnia. From the digestive tract: - diarrhea (diarrhea); - increased appetite; - nausea, sometimes vomiting. From the side of the eyes – exophthalmos (bulging eyes).
Myxedema.
This is a disease that is manifested by a decrease in the level of thyroid hormones. Clinically manifested by signs of hypothyroidism. Due to the development of swelling in the tissues, the disease got its name - “mucosal edema”. Myxedema develops due to the cessation (or reduction) of the thyroid gland’s production of its hormones. Occurs when: - inflammation of the thyroid gland; — autoimmune damage to the thyroid gland; - tumor of the thyroid gland. And, often, a decrease in the production of thyroid hormones occurs when the hormonal control of the pituitary gland is disrupted. Stress, nervous strain, and mental disorders cause disruption of TSH production. Without the stimulating effect of TSH, the thyroid gland does not produce the required amount of hormones. Myxedema manifests itself: - drowsiness; - dry skin; - pale skin; - swelling on the face and limbs; - brittle hair and nails; - bradycardia - slowing of cardiac activity; - lowering blood pressure; - decrease in body temperature; - constipation; - increase in body weight. A very common type of thyroid disease is autoimmune thyroiditis or Hashimoto's disease. The disease occurs as a breakdown of the immune system, in which one’s own immunity (leukocytes) attacks the tissue of one’s own thyroid gland. Hashimoto’s thyroiditis manifests itself with a slow course and moderate manifestations of hypothyroidism. The disease can last for years, giving minor manifestations.
Treatment of thyroid diseases.
There are two options for treating the thyroid gland - conservative and surgical. Conservative treatment 1. The use of iodine preparations is very important and advisable. Especially with endemic goiter. Additional administration of iodine reduces the need for the gland and improves its functioning. This is one of the important factors in the prevention of thyroid diseases. 2. Thyroid hormone preparations – L-thyroxine, eutirox. Used as replacement therapy for hypothyroidism. 3. Antithyroid drugs - Mercazolil and its analogues. Used to reduce the effect of thyroid hormones in hyperthyroidism. 4. Hormonal anti-inflammatory drugs (steroids) – prednisolone. Used to reduce the manifestations of inflammation in Hashimoto's autoimmune thyroiditis. Surgical treatment consists of two types of operations: 1) hemithyroidectomy - removal of half of the thyroid gland, which contains nodes and cysts. 2) thyroidectomy – complete removal of the thyroid gland. In this case, the parathyroid glands are necessarily left behind. Surgical treatment is carried out: - if conservative treatment of diffuse toxic goiter is ineffective; — in the presence of large nodes and the risk of developing oncological complications (it should be taken into account that a node is an area of poor blood supply, it is a source of cancer cells); - when the goiter compresses the larynx and trachea (difficulty breathing); After removal of the thyroid gland, postoperative hypothyroidism always develops (insufficient levels of thyroid hormones in the body). The patient is forced to take hormonal medications throughout his life and continues to live for many years.
Diagnosis of thyroid goiter
Based on the size of the enlarged thyroid gland, goiter is divided into three degrees:
- zero - normal size, when each of the two lobes is no larger than the nail phalanx of the patient’s thumb;
- the first provides two options - the node does not change the size of the lobe or there is a diffuse increase to the touch, but visually imperceptible;
- second, the gland is visible to the naked eye.
In most cases, nodes are found by chance, by palpation or during ultrasound of the neck for another clinical reason. A one-centimeter node can already be felt. The leading method for diagnosing organ pathology is ultrasound .
CT is used when the gland is very large and to detect a lobe hidden behind the sternum, which can cause complaints of pressure and breathing problems. People with very short necks may develop a substernal goiter. MRI today is not considered a competitor to ultrasound and CT and is considered less informative.
To identify functional capabilities, all patients with pathology undergo a blood test for the content of gland hormones and the stimulator of their production - pituitary thyroid-stimulating hormone or TSH. Blood calcitonin must be determined , which increases significantly in medullary cancer. If the calcitonin level is from 60 to 100 pg per milliliter of blood, then stimulation with calcium gluconate will help determine the diagnosis.
The next mandatory stage of diagnosis is fine- needle aspiration biopsy or FNA, which allows one to fairly accurately determine the nature of the process. In fact, this is a puncture of a pathological focus with a gradation of findings during microscopy according to Bethesda categories.
A biopsy is not always done, but for nodes larger than 1 centimeter it is required:
- for young people - under 20 years of age;
- with signs of a malignant process according to ultrasound data in the nodal formation itself or in the cervical lymph nodes;
- with a high concentration of calcitonin, characteristic of medullary carcinoma;
- with a family history of thyroid cancer;
- long-standing irradiation of the neck due to some other disease;
- The immobility of one vocal cord and the glow of the node on PET, performed for another clinical reason, are alarming for malignancy.
Isotope examination of the thyroid gland is not always carried out; scanning is necessary and useful:
- with its hyperfunction;
- the location of glandular tissue not only in the gland, but also in other organs - ectopic tissue.
Classification of the disease
Types of goiter by morphology
Diffuse goiter
Diffuse toxic goiter is a disease of the endocrine system in which the thyroid gland increases in size and secretes an increased amount of hormones. Impairment of organ function most often results from insufficient intake of such an important microelement as iodine. Other factors also contribute to the development of the disease: heredity, inflammatory diseases, trauma to thyroid tissue, autoimmune processes, poor environmental conditions, and frequent stress.
Symptoms of diffuse goiter are most often observed in women aged 30 to 50 years. The disease is 8 times less common in men. In some cases, a malfunction of the gland may be diagnosed in childhood or in old age. If the tissues of the organ grow evenly, they speak of an endemic type of disease; in the presence of local formations, the goiter is called diffuse nodular.
The degrees of diffuse toxic goiter vary depending on the severity of the proliferation of thyroid tissue. At the initial stage, the disease can only be detected by ultrasound; at the second stage, there are usually symptoms such as a feeling of interference, a coma in the throat and others. In a later period, the goiter increases significantly in size and appears as a tumor on the front of the neck.
Treatment of diffuse toxic goiter is carried out by an endocrinologist. For minor disorders and for prevention, patients are prescribed medications containing iodine and a special diet. If the thyroid gland is significantly enlarged, tests are performed to monitor hormonal levels. Drug therapy consists of correcting it and maintaining normal levels. In some situations, the doctor may prescribe radioiodine therapy, in which radioactive iodine is introduced into the body, which accumulates in the cells of the thyroid gland and exposes the entire gland to radiation, destroying tumor cells and thyroid cells. In difficult cases, with significant tissue growth and the ineffectiveness of conservative treatment methods, surgery to remove the tumor may be prescribed.
Nodular goiter
Nodular goiter is a disease that covers all isolated formations in the tissues of the thyroid gland. The formations can be of any size and have a capsule. Nodes are determined visually or by palpation. The reasons for the formation of a multinodular goiter can be different.
Formations in tissues can be single or multiple, separately located or communicating. They can be of different sizes and different densities.
Treatment of nodular goiter is carried out in cases where the functioning of the thyroid gland is disrupted or the formation is large and interferes with the normal functioning of neighboring organs. Depending on the diagnostic results, treatment may involve regulating hormone levels or removing overgrown tissue.
Diffuse nodular goiter
A mixed form of goiter, combining the features of diffuse and nodular goiter. With this disease, both the tissues of the thyroid gland themselves grow, and the appearance of individual tumors - nodes - is observed in it.
Treatment of diffuse nodular goiter is carried out with hormonal and iodine-containing drugs, in some cases surgery is prescribed.
Types of goiter according to etiopathogenetic classification
Endemic goiter
A disease that is caused by a chronic lack of iodine in the body due to low iodine content in food, water, air and soil. It is more common among mountain residents. This leads to the growth of thyroid tissue and changes in its functioning. If there is a lack of iodine, the thyroid gland needs to take more iodine from the blood to function. Endemic goiter is promoted by genetic predisposition and defects, heredity, poor ecology, lack of iodine in the environment, infectious and inflammatory processes, taking medications that block iodide transport or disrupt the organization of iodine in the thyroid gland.
Sporadic goiter
A disease of the thyroid gland that occurs in residents of regions where there is sufficient iodine content in the air, water, food and soil.
Types of goiter by localization
- With the usual arrangement;
- Annular;
- Partially substernal;
- Dystopic goiter from embryonic anlages.
Types of goiter by functionality
Euthyroidism
A goiter in which the thyroid gland is functioning normally. Thyroid hormones and thyroid-stimulating hormone of the pituitary gland in the blood are at normal levels.
Thyrotoxicosis
Goiter, in which the thyroid gland produces an increased amount of thyroid hormones. In this case, increased metabolism occurs, and even with overeating, a person with thyrotoxicosis can lose weight. Symptoms of this disease include rapid heartbeat, weight loss, frequent bowel movements, increased sweating, impaired memory and attention, decreased libido and restlessness.
Hypothyroidism
Goiter, in which the thyroid gland does not produce enough thyroid hormones. Metabolism slows down and the person begins to gain weight. Symptoms of this disease include decreased performance, slowness, lethargy, fatigue, memory loss, drowsiness, decreased appetite, a feeling of chilliness, bowel movements, constipation and others.
Goiter degrees
WHO classification of goiter:
- Grade 0 - no goiter.
- Degree 1 - the goiter is palpable, but not visible to the eye with the neck in normal position.
- Degree 2 - the goiter is palpable and easily detected visually.
Classification of goiter according to O. V. Nikolaev:
- Grade 1 - the goiter is palpable.
- Degree 2 - goiter is determined visually.
- Grade 3 - the neck is enlarged.
- Grade 4 - the shape of the neck is changed.
- Degree 5 - goiter of gigantic size.
The first signs and symptoms of thyroid goiter
The vast majority of patients do not have any symptoms if hormone production is normal. Enlargement of the lower third of the neck is possible with diffuse or multinodular goiter; individual nodules up to a centimeter do not change the configuration of the neck.
Compression of the trachea is possible if the trachea is very large or if the main mass of glandular tissue is located behind the sternum, as well as an increase in the diameter of the cervical vessels and a change in voice to the point of hoarseness.

Inadequate production of hormones does not correlate with the size of the gland and nodes; the symptoms of thyrotoxicosis or hypothyroidism are not obvious and nonspecific, but are manifested by impaired functioning of target organs: the cardiovascular system, nervous, subcutaneous fat, skin and muscles.
Initially, the patient complains of palpitations, nervousness, difficulty sleeping and concentration, weight loss or gain. A cardiac examination that does not detect cardiac pathology is performed, and only a blood test reveals abnormal hormone levels.
Very rarely, the classic thyrotoxic triad occurs: palpitations with trembling and exophthalmos - bulging eyes. An elderly patient may be hospitalized with thrombosis and heart rhythm disturbances with a visually undetectable pathology, but releasing too many hormones.
It is very rare that an adenoma develops that produces excess thyroid hormones; almost 80% of thyrotoxicosis is caused by a diffuse increase.
Treatment methods
Treatment is required only for goiter symptoms. Thus, thyrotoxicosis with a diffuse increase is treated with goitrogenic drugs that suppress the synthesis of hormones, or the producing adenoma is removed. Insufficient function, on the contrary, is compensated for by synthetic endocrine drugs.
Nodular goiter cannot be treated with any medications; removal of a benign neoplasm is necessary:
- if you suspect cancer;
- compression of surrounding structures by the mass of the gland;
- life-impairing cosmetic neck deformity;
- if it is impossible to use radioactive iodine in a patient with thyrotoxicosis.
In other cases, with a node less than a centimeter, the patient is monitored with annual blood tests and ultrasound. For “goitrogenic” risk factors, examinations are carried out every six months. The growth of a node between examinations is a reason for a biopsy.
The question of surgery is raised when cellular atypia is detected, since cancer can occur under its mask in 30% of cases. The cytological picture of “follicular neoplasia”, and even more so “suspicion of cancer”, is the basis for removal of the affected lobe - hemithyroidectomy.
Treatment with radioactive iodine is highly effective; in case of thyrotoxicosis, hormone production returns to normal within a month. Contraindicated only for pregnant and lactating women, unacceptable in case of decreased function.
Indications for radioiodine therapy:
- obligatory when the thyroid gland is “uncontrolled” by pituitary hormones - an autonomous function with hyperproduction;
- possible for nodes with contraindications to surgery.
If the patient is unable or unwilling to undergo surgery, and the benign nature of the process is absolutely proven, innovative alternative methods are possible:
- introduction of sclerosing substances into the node - alcohol, tetracycline and others;
- destruction of the node by laser, liquid nitrogen, electric current.
Hirudotherapy does not stand up to criticism; the folk method does not cure goiter. The thyroid gland is abundantly supplied with blood, leeches are promised abundant nutrition, but they are not able to change the pathological structure. Nodular goiter cannot be cured with any medications; the node can only be removed.
Treatment
Goiter is suspected if the patient complains of weight problems, palpitations, sleep disturbances, nervousness and other symptoms. but these symptoms may indicate other diseases. For an accurate diagnosis, the patient is examined.
Diagnostics
The following methods are used to diagnose goiter:
- Visual inspection of the patient's neck. The gland is visible only in grade 2 goiter.
- Feeling the thyroid gland:
- with zero degree goiter, the thyroid gland is in normal condition;
- in the first degree of goiter, the thyroid gland is not visible, but its diffuse enlargement is palpable.
- Ultrasound. Allows you to more accurately determine even small nodes in the thyroid gland.
- CT. Used to diagnose substernal goiter and large thyroid gland.
- Blood test for thyroid hormone levels.
- Thyroid puncture for biopsy. As a rule, it is done for nodes larger than 1 centimeter and if the process is suspected of being of poor quality. Allows you to determine the type of tumor.
After diagnosing goiter and obtaining accurate data about the disease, drug therapy or surgery is prescribed.
Therapy
In case of thyrotoxicosis, when the thyroid gland produces an increased amount of thyroid hormones, goitrogenic drugs are prescribed that reduce the production of hormones.
In case of hypothyroidism, when the thyroid gland produces an insufficient amount of thyroid hormones, synthetic endocrine drugs are prescribed to replenish the lack of hormones in the body.
Some types of goiter are treated with radioiodine therapy. This procedure involves injecting radioactive iodine, which accumulates in the thyroid cells and exposes the entire gland to radiation, destroying tumor cells and thyroid cells. Radioiodine therapy is usually used in the treatment of thyrotoxicosis accompanying diffuse toxic goiter and adenomas.
Operation
Surgical removal of goiter is prescribed for:
- When the goiter puts pressure on the surrounding tissues of the body;
- If a malignant tumor of the thyroid gland is suspected;
- If there is a deformation of the neck that prevents the patient from living a normal life;
- If it is impossible to use radioiodine therapy.
Depending on the patient’s condition and the type of disease, one lobe of the thyroid gland can be removed - hemithyroidectomy, or two lobes of the thyroid gland can be removed - subtotal resection. With complete removal, the surgeon leaves parts of the thyroid tissue, the weight of which is less than 6 grams of the original weight of the lobes. Rarely, absolutely all thyroid tissue is removed - thyroidectomy.
The operation can be:
- Conventional with a large incision through which the surgeon gains access to the organ;
- Endoscopic, with small incisions through which endoscopic instruments are inserted.
The surgical method is chosen by the surgeon depending on the patient’s condition.
You can make an appointment for diagnosis and treatment of goiter at our L-Med clinic by calling +7 (4872) 49-57-57
or through the online form on the website.
Complications
Surgical treatment helps to get rid of a nodular goiter suspicious for a malignant process, but is associated with complications, infrequent, but nevertheless unpleasant:
- damage to the laryngeal nerve with subsequent hoarseness,
- removal of the parathyroid gland responsible for calcium metabolism,
- relapse of goiter.
The frequency of complications is affected by the size of the enlarged gland; the larger, the more likely it is. However, the incidence of complications does not exceed one percent.
But the most common complication of surgery and radioactive iodine is insufficiency of endocrine function, that is, a decrease in the level of thyroid hormones below the critical level, which is compensated by lifelong use of hormonal drugs.
Autoimmune thyroiditis - symptoms and treatment
Therapy for autoimmune thyroiditis of the thyroid gland is nonspecific. When the phase of thyrotoxicosis develops, the use of symptomatic therapy is sufficient. When hypothyroidism develops, the main option for drug therapy is the administration of thyroid hormones. Now in the pharmacy chain of the Russian Federation it is possible to purchase only Levothyroxine sodium tablets (L-thyroxine and Euthyrox). The use of tableted preparations of thyroid hormones neutralizes the clinical picture of hypothyroidism and, in the hypertrophic form of autoimmune thyroiditis, causes a decrease in the volume of the thyroid gland to acceptable values.
If a patient has manifest hypothyroidism (an increase in the level of thyroid-stimulating hormone and a decrease in the concentration of free T4), it is necessary to use levothyroxine sodium in the treatment at an average dose of 1.6 - 1.8 mcg/kg of the patient’s body weight. An indicator of the correctness of the prescribed treatment will be the confident retention of thyroid-stimulating hormone in the patient’s blood within the reference values.
When a patient is diagnosed with subclinical hypothyroidism (increased TSH concentration in combination with unchanged free T4 concentration), it is necessary:
- After 3–6 months, carry out a second hormonal examination to confirm the presence of changes in thyroid function;
- When an increase in thyroid-stimulating hormone levels is detected in a patient during pregnancy, even with preserved free T4 concentrations, prescribe levothyroxine sodium at the full calculated replacement dose immediately;
- Treatment with levothyroxine sodium is necessary for persistent subclinical hypothyroidism (an increase in the concentration of thyroid-stimulating hormone in the blood above 10 mU/l, and also in situations of at least twice the determination of the concentration of thyroid-stimulating hormone between 5 - 10 mU/l), but if these patients are over 55 years old and have they have cardiovascular pathologies, treatment with sodium levothyroxine is prescribed only if the drug is well tolerated and in the absence of information about decompensation of these diseases while taking thyroxine;
- An indicator of the sufficiency of treatment for subclinical hypothyroidism is the stable maintenance of TSH levels within the reference values in the blood.
If women, before planning pregnancy, have antibodies to thyroid tissue and/or ultrasound signs of autoimmune thyroiditis, it is necessary to determine the hormonal function of the thyroid gland (thyroid-stimulating hormone concentration and free T4 concentration) and be sure to determine the level of hormones in each trimester of pregnancy.[8]
If autoimmune thyroiditis is diagnosed, but changes in the functioning of the thyroid gland are not detected, the use of sodium levothyroxine is not indicated.[9] It is sometimes possible in exceptional situations of an impressive increase in the volume of the thyroid gland, provoked by autoimmune thyroiditis, and the decision is made for each patient individually.[10]
Physiological amounts of potassium iodite (approximately 200 mcg/day) cannot provoke the formation of hypothyroidism and do not have a negative effect on thyroid function in previously developed hypothyroidism caused by autoimmune thyroiditis.
Nutrition for autoimmune thyroiditis
There are no products that affect the course of autoimmune thyroiditis. Gluten or lactose are not related to hypothyroidism due to AIT. Therefore, dietary recommendations for people with autoimmune thyroiditis are the same as for everyone else: a varied, balanced diet with sufficient water intake.
Are there traditional methods of treatment?
Autoimmune thyroiditis is treated only with medications prescribed by an endocrinologist. The lack of adequate therapy can lead to dangerous complications: impaired reproductive function, severe memory loss (even dementia), anemia and coma, which occurs with a severe deficiency of thyroid hormones.
Goiter prevention
There is no region in Russia where the population does not experience iodine deficiency, so the consumption of iodized products, primarily salt, is very important for the health of the thyroid gland. In endemic areas, it is useful to take iodine preparations; for an adult, 120 mcg of iodine is needed daily, for pregnant and lactating women - 250 mcg.
Surgeries on the neck organs require extensive surgical experience and technical virtuosity; the surgeons and oncologists of our clinic have created all the conditions for high-quality care for our patients.
Book a consultation 24 hours a day
+7+7+78