Platelet shapes
There are 5 forms of platelets:
1) young (0-0.8%);
2) mature (90.1 -95.1%);
3) old (2.2-5.6%);
4) forms of irritation (0.8-2.3%);
5) degenerative forms (0-0.2%).
Platelet morphology
Unactivated platelets circulating in the blood, to a first approximation, are oblate spheroids with a semi-axial ratio from 2 to 8, and a characteristic size of 2-4 μm in diameter [1]. This approximation is often used when modeling the hydrodynamic and optical properties of a platelet population, as well as when reconstructing the geometric parameters of individual measured platelets using flow cytometry methods[2]. Confocal microscopy data[3] indicate that a change in the shape of a platelet during its activation is associated with a change in the geometry of the microtubule ring, which in turn is caused by a change in the concentration of calcium ions. More accurate biophysical models of platelet surface morphology, modeling its shape from first principles, make it possible to obtain a more realistic geometry of platelets in a quiet and activated state [4] than an oblate spheroid.
Leukocytes
White blood cells (L, WBC) are blood cells produced in the bone marrow and lymph nodes. There are 5 types of leukocytes: granulocytes (neutrophils, eosinophils, basophils), monocytes and lymphocytes. The main function of leukocytes is to protect the body from foreign antigens (including microorganisms, tumor cells; the effect also manifests itself in the direction of transplant cells).
Normal leukocyte content in the blood: (4-9) x 109
Leukocytosis is an increased level of leukocytes in the blood.
Leukopenia is a decrease in the number of leukocytes in the blood.
Functions
Scanning electron micrograph (SEM) of human blood cells: red blood cell, activated platelet, white blood cell (from left to right)
Platelets have two main functions:
- Formation of a platelet aggregate, a primary plug closing the site of vessel damage;
- Providing its surface to accelerate key plasma coagulation reactions.
Relatively recently, it was found that platelets also play a critical role in the healing and regeneration of damaged tissues, releasing growth factors into damaged tissues that stimulate cell division and growth. Growth factors are polypeptide molecules of various structures and purposes. The most important growth factors include platelet-derived growth factor (PDGF), transforming growth factor (TGF-β), vascular endothelial growth factor (VEGF), epithelial growth factor
(EGF), fibroblast growth factor (FGF),
insulin-like growth factor
(IGF)[5].
The physiological plasma concentration of platelets is 180-360*10^9 platelets per liter.
A decrease in the number of platelets in the blood can lead to bleeding. An increase in their number leads to the formation of blood clots (thrombosis), which can block blood vessels and lead to pathological conditions such as stroke, myocardial infarction, pulmonary embolism, or blockage of blood vessels in other organs of the body.
A deficiency or disease of platelets is called thrombocytopathy, which can be either a decrease in the number of platelets (thrombocytopenia), a violation of the functional activity of platelets (thrombasthenia), or an increase in the number of platelets (thrombocytosis). There are diseases that reduce platelet counts, such as heparin-induced thrombocytopenia or thrombotic purpura, which usually cause thrombosis instead of bleeding.
Due to the inaccuracy of descriptions, the lack of photographic equipment and the confusing terminology of the early periods of the development of microscopy, the exact time of the first observation of platelets is unknown. Most often, their discovery is attributed to Donna (1842, Paris), but there is evidence that they were observed by Anthony van Leeuwenhoek (1677, the Netherlands). The term “blood platelets,” which is still preferred in English-language literature (blood platelets), was introduced by Bizzocero (1881, Turin), who also played a leading role in identifying the connection of platelets with homeostasis and thrombosis. This subsequently led to the emergence of the term “platelet” (Dekhuizen, 1901), which became the main one in the Russian language. In the English-language literature, the term is used exclusively for nucleated platelets in non-mammalians (thrombocytes). In addition, in Russian literature the term “Bizzocero plaque” may be used for platelets.
Hemoglobin
Hemoglobin (Hb, Hgb) in a blood test is the main component of red blood cells, which transports oxygen from the lungs to organs and tissues. For analysis, a cyanide complex or cyanide-free reagents are used (as a replacement for toxic cyanide). It is measured in moles or grams per liter or deciliter. Its definition has not only diagnostic, but also prognostic significance, since pathological conditions leading to a decrease in hemoglobin content lead to oxygen starvation of tissues.
The normal hemoglobin content in the blood is:
- men - 135-160 (130-170) g/l (grams per liter);
- women - 120-140 (120-150) g/l;
- children - 120-140 g/l.
Anemia (low hemoglobin) - a decrease in the total amount of hemoglobin in the blood.
Hyperchromemia (high hemoglobin) is an increase in the concentration of hemoglobin in the blood.
Participation in folding
A special feature of the platelet is its ability to activate - a rapid and, as a rule, irreversible transition to a new state. The activation stimulus can be almost any environmental disturbance, even simple mechanical stress. However, the main physiological activators of platelets are collagen (the main protein of the extracellular matrix), thrombin (the main protein of the plasma coagulation system), ADP (adenosine diphosphate, appearing from destroyed vascular cells or secreted by the platelets themselves) and thromboxane A2 (a secondary activator synthesized and released by platelets; its additional function is to stimulate vasoconstriction).
Activated platelets become able to attach to the site of damage (adhesion) and to each other (aggregation), forming a plug that covers the damage. In addition, they participate in plasma coagulation in two main ways - exposure of the procoagulant membrane and secretion of α-granules.
Sequence of primary biochemical and morphological changes upon activation
The initial stages of platelet activation under the influence of external factors are associated not only with the appearance of biochemical markers, but also with morphological changes in the form of the platelet. As has been shown by flow cytometry and electron microscopy, the most sensitive sign of activation (when platelets are exposed to ADP) are morphological changes[6]. The appearance of biochemical and morphological changes, arranged according to the degree of decrease in sensitivity, is as follows: change in platelet shape, conformational changes in glycoprotein IIb/IIIa, expression of P-selectin, expression of phosphatidylserine.
Exposure of the procoagulant membrane
Under normal conditions, the platelet membrane does not support clotting reactions. Negatively charged phospholipids, primarily phosphatidylserine, are concentrated in the inner layer of the membrane, while phosphatidylcholine in the outer layer binds coagulation factors much less well. Although some coagulation factors can bind to non-activated platelets, this does not lead to the formation of active enzymatic complexes. Activation of the platelet presumably leads to the activation of the scramblase enzyme, which begins to quickly, specifically, bidirectionally and ATP-independently transfer negatively charged phospholipids from one layer to another. As a result, thermodynamic equilibrium is established, in which the concentration of phosphatidylserine in both layers is equalized. In addition, upon activation, many transmembrane proteins in the outer layer of the membrane undergo alignment and/or conformational changes, and they acquire the ability to specifically bind coagulation factors, accelerating reactions involving them.
Platelet activation has several degrees, and procoagulant surface expression is one of the highest. Only thrombin or collagen can produce such a strong response. A weaker activator, especially ADP, can contribute to the work of stronger activators. However, they are not able to independently cause the appearance of phosphatidylserine; their effects are limited to changes in platelet shape, aggregation and partial secretion.
Secretion of α-granules
Platelets contain several types of granules, the contents of which are secreted during activation. Essential for coagulation are α-granules containing high molecular weight proteins such as factor V and fibrinogen.
Thrombocytopenia: symptoms and treatment
How to determine?
If a laboratory blood test reveals a significant decrease in the number of platelets compared to age norms, the child is diagnosed with thrombocytopenia.
This condition is dangerous for a small organism, since if the epithelium is damaged or internal bleeding occurs, the blood cannot clot, which leads to significant blood loss and a sharp deterioration in well-being (in some cases, even death).
The only way to stop the bleeding may be a transfusion of donor blood with a high platelet count.
To prevent serious consequences, it is important to know the symptoms and signs of thrombocytopenia in children. These include:
- frequent nosebleeds;
- bleeding gums, independent of tooth brushing;
- bruises and small hematomas on the body;
- a small rash that occurs mainly on the legs, ankles, thighs and buttocks (appears in 100% of children with this diagnosis);
- blood streaks in feces and urine.
Separately, it is worth paying attention to cases when even with minor damage to the skin (for example, with a shallow cut), a large amount of blood is observed. This sign almost 100% indicates developing thrombocytopenia.
Causes
A decrease in platelets is not always caused by internal pathologies. There are also external reasons for which signs of thrombocytopenia may be observed in children.
Tests to evaluate the vascular-platelet component of hemostasis
- Bleeding time;
- The number of platelets in the blood;
- Induced platelet aggregation.
Qualitative platelet defects, which underlie a large number of hemorrhagic diathesis, are divided into the following groups:
- disaggregation thrombocytopathies caused by the absence or blockade of platelet membrane receptors (Glanzmann’s thrombasthenia, etc.);
- diseases of the absence of dense and α-granules;
- granule release disorders;
- disturbances in the formation of cyclic prostaglandins and thromboxane A2;
- deficiency, anomalies and disorders of the multidimensionality of von Willebrand factor;
- disorders of nucleotide metabolism and calcium transport.
Decoding the PCT indicator in a blood test
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
The PCT value in a blood test allows you to determine the quantitative content of platelets. The purpose of counting blood cells is to establish thrombocytopenia, which can be hypoproliferative and hyperdestructive. Platelet indices are a simple diagnostic method that has become available through automatic cell counting.
PCT indicator in blood test
Thrombocrit refers to the percentage of platelet mass in the blood volume. Deviation from the norm is a prerequisite for further research. It is important to compare the obtained value with the number of platelets responsible for the coagulation indicator in a general blood test.
Our readers successfully use ReCardio to treat hypertension. Seeing how popular this product is, we decided to bring it to your attention. Read more here...
The level decreases against the background of B12 deficiency, folic acid, as well as in hematopoietic disorders (Fanconi and aplastic anemia), viral infections, leukemia and granulomatosis after taking corticosteroids and cytostatics. An increase is observed in immune thrombocytopenic purpura, but more often in diseases of the cardiovascular system. Inflammatory processes and infections, tuberculosis, tumors, blood loss, ulcers and necrosis, anemia and diabetes mellitus, and surgical interventions can change the indicator upward. Platelets are important for wound healing because they help:
- stop blood loss;
- stimulate tissue regeneration.
Platelet indices are useful markers for the early diagnosis of thromboembolic diseases. Thrombocrit is considered together with two other indicators - the average volume and range of platelet distribution. Their values make it possible to identify the causes of thrombocytopenia, as well as to determine immune thrombocytopenic purpura.
The range of platelet distribution increases due to their activation with an increase in cell volume and the formation of pseudopodia. An increase in the average value is associated with the following conditions:
- inflammatory processes in the intestines;
- immune thrombocytopenic purpura;
- myeloproliferative diseases;
- preeclampsia and recovery from hypoplasia.
A decrease in the level of blood platelets occurs against the background of bleeding.
Analysis transcript
Thrombocrit is normally between 0.2 and 0.36%, but is not considered alone.
It is necessary to focus on the platelet indices presented in the table:
Platelet crit (PCT)0.2–0.36%.Mean platelet volume (MPV)7–10 femtolitersPlatelet distribution range (PDW)56.6%A blood test with PCT decoding is useful to confirm certain diseases:
- suspicion of sepsis and determination of its danger;
- severe bacterial infections and their complications;
- unknown fevers;
- suspicion of meningitis, peritonitis and pneumonia.
The indicator helps to evaluate the effectiveness of therapy in shock, sepsis, immunosuppression and neutropenia, after organ transplantation and spleen removal, while on a ventilator.
Factors influencing the indicator
Thrombocrit, by analogy with hematocrit, determines the mass of settled cells. Platelets in the external environment undergo changes: they form pseudopodia, increase in size, stick together or undergo aggregation, and therefore they are difficult to count. After the development of automatic blood analyzers, this became much easier, which is why thrombocrit appeared in the list of research results. The number of platelets is counted only as directed by a doctor, since the process requires the use of special conditions and reagents.
A false decrease in thrombocrit may be due to the following factors:
- Partial clotting of a blood sample with platelet activation and aggregation during injection.
- Platelet aggregation when using ethylenediaminetetraacetic acid (EDTA) as a stabilizer.
- Platelet satellitetism, or their adherence to neutrophils when using various anticoagulants for analysis, which is associated with the production of IgG or IgM antibodies.
- Detection of giant cells that cannot be identified by automatic counters.
A false increase in level occurs against the background of the following conditions:
- Fragmentation of red blood cells, when small cells or their fragments were counted as platelets.
- Cryoglobulinemia (detection of immunoglobulins in serum) is associated with pseudothrombocytosis and pseudoleukocytosis.
Low and high values are confirmed with a repeat blood test.
Differences in thrombocrit levels for children and adults are not clinically determined. All platelet indices generally change proportionally with age, and PCT is determined by multiplying mean platelet volume (MPV) by cell count.
It is necessary to pay attention to fluctuations in the number of platelets, which can be physiological and pathological. The indicator is influenced by the following factors:
- In the spring and during depression, as well as at night, the level of platelets and thrombocrit decreases by 10% compared to normal.
- During menstrual bleeding and pregnancy, the norm in women decreases by 50%.
- Thrombocrit doubles after exercise.
Reasons for deviation from the norm
The thrombocrit indicator determines the risk of bleeding and thrombosis - conditions that threaten a person’s life. The blood cell ratio reveals hematopoietic disorders or hidden pathologies that cause the body to produce more platelets.
An increased level of thrombocrit is characteristic of the following pathologies:
- hyperthyroidism and diabetes mellitus;
- atherosclerosis, heart attacks and strokes;
- iron deficiency anemia (a common cause in children);
- viral and inflammatory processes;
- myeloproliferative diseases.
Smoking also increases your PCT score.
A sharp decrease in thrombocrit means a severe hematological condition - thrombocytopenia, which is associated with two pathologies:
- damage to the megakaryocyte lineage, leading to reduced production of blood cells;
- accelerated destruction and utilization of platelets.
The cause of low thrombocrit is blood diseases, chronic pathologies of internal organs and conditions that affect cellular functions. Low thrombocrit indicates or confirms the following ailments:
- megaloblastic and aplastic anemia;
- viral infections;
- liver cirrhosis and renal failure;
- intoxication;
- tumors of lymphoid and hematopoietic tissues;
- autoimmune lesions of connective tissues.
Under the influence of radiation, chemotherapy and prolonged use of antibiotics, the PCT value also changes.
Notes
- M. M. Frojmovic, R. Panjwani.
Geometry of normal mammalian platelets by quantitative microscopic studies // Biophysical Journal. — 1976-09. - T. 16, issue. 9. - pp. 1071–1089. — ISSN 0006-3495. - doi:10.1016/s0006-3495(76)85756-6. - Alexander E. Moskalensky, Maxim A. Yurkin, Valeri P. Maltsev, Elena D. Chikova, Galina A. Tsvetovskaya, Andrei V. Chernyshev, Vyacheslav M. Nekrasov.
Accurate measurement of volume and shape of resting and activated blood platelets from light scattering // Journal of Biomedical Optics. - 2013/01. - T. 18, issue. 1. - P. 017001. - ISSN 1083-3668 1560-2281, 1083-3668. - doi:10.1117/1.JBO.18.1.017001. - Karin Sadoul, Saadi Khochbin, Jin Wang, Arnold Fertin, Alexei Grichine.
Motor-driven marginal band coiling promotes cell shape change during platelet activation // J Cell Biol. — 2014-01-20. - Vol. 204, iss. 2. - P. 177–185. — ISSN 0021-9525 1540-8140, 0021-9525. - doi:10.1083/jcb.201306085. - Alexander E. Moskalensky, Maxim A. Yurkin Valeri P. Maltsev, Andrei V. Chernyshev, Vyacheslav M. Nekrasov, Alena L. Litvinenko, Artem R. Muliukov.
Method for the simulation of blood platelet shape and its evolution during activation (English) // PLOS Computational Biology. — 2018-03-08. - Vol. 14, iss. 3. - P. e1005899. — ISSN 1553-7358. - doi:10.1371/journal.pcbi.1005899. - University of Michigan, USA.
Platelet Rich Plasma: Myth or Reality? (English). Access date: February 3, 2010. - Rustem I. Litvinov, John W. Weisel, Izabella A. Andrianova, Alina D. Peshkova, Giang Le Minh.
Differential Sensitivity of Various Markers of Platelet Activation with Adenosine Diphosphate (English) // BioNanoScience. — 2018-12-10. — P. 1–6. — ISSN 2191-1630 2191-1649, 2191-1630. - doi:10.1007/s12668-018-0586-4.
Mean platelet volume (MPV)
The average platelet volume ranges from 3.5 – 9.5 µm^3 (7-10 fl)
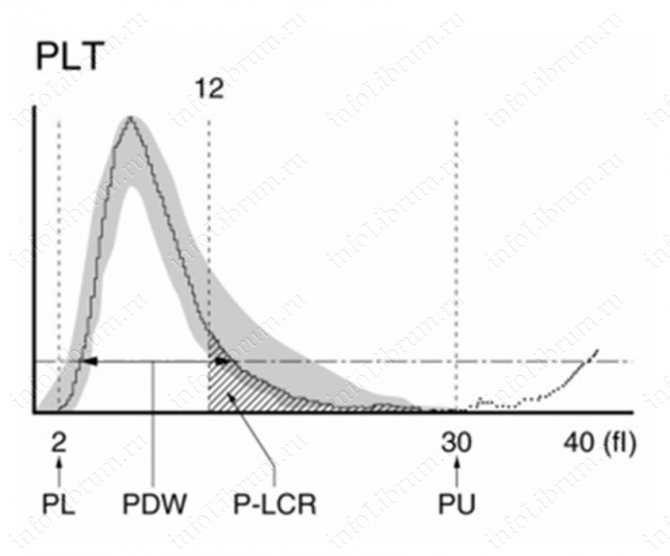
During a general blood test, a histogram of platelet distribution over the volume of the material being studied is constructed, with the priority of young platelets shifting the histogram to the right, while the priority of old platelets shifts the histogram to the left (the volume of the old platelet is less than the volume of the young). Bernag-Soulier syndrome and May-Hegglin anomaly lead to an increase in the average platelet volume, and Wiskott-Aldrich syndrome causes a decrease.
Poikilocytosis
Poikilocytosis is a pathological modification of red blood cells. In this case, cellular deformation and improper functioning occur.
The presence of cells means the presence in the body of one or another type of anemia, which in most cases has a moderate or severe stage.
To detect poikilocytosis of red blood cells, a general blood test is performed. If the result indicates the presence of “anisocytosis” or “poikilocytosis” on the form, further verification will be required.
At the first concept, possible initial stage anemia. that the patient suffers from mild anemia. Poikilocytosis may indicate a moderate to severe stage.