There are several chords in the human heart that prevent the valve from bending during contraction of this organ. Thanks to their presence, it retains blood well and ensures adequate hemodynamics. The normal chord is a kind of spring with a muscular structure. Sometimes during intrauterine development, an additional chord appears in one of the ventricles of the heart, which is a thread-like cord of connective tissue. In some cases, this abnormal formation includes muscle or tendon fibers.
In this article we will look at such a minor cardiac anomaly as an accessory chord of the left ventricle. In most cases, it is found in children under 18 years of age, but some people live with this diagnosis for many years and do not feel any changes in the functioning of the heart. Usually, an additional chord is detected by chance: during an examination for another disease or during a preventive examination. It is not detected either by listening to a heart murmur or by an ECG, and an accurate diagnosis can only be made after an ECHO-CG. Having heard a heart murmur, the doctor can only suspect the presence of this minor heart anomaly and recommend an ultrasound examination to refute or confirm the diagnosis.
In our article we will introduce you to the causes of development, types, symptoms, methods of observation, treatment and prevention of accessory chord of the left ventricle. This knowledge will help parents of children with such a heart anomaly choose the right tactics to approach the problem and save them from unnecessary worries.
Causes
An abnormal chord of the left ventricle is a hereditary anomaly, which in 92% of cases is inherited through the maternal line (in rare cases, through the paternal line), and develops in utero due to a failure in the development of connective tissue. That is why mothers who have previously been diagnosed with this disease are recommended to have their child examined.
It is possible that the following unfavorable factors may be the reasons for the appearance of an additional chord:
- bad ecology;
- smoking or drinking alcohol and drugs;
- nervous and physical stress.
Clinical significance of minor cardiac anomalies in children
In recent years, much attention has been paid to connective tissue dysplasia (CTD) in children. DTD is understood as a congenital anomaly of the connective tissue structure of various organs and systems, which is based on a decrease in the content of certain types of collagen and/or a violation of their ratio, leading to a decrease in the strength of connective tissue [12, 13, 24, 26].
Endogenous (chromosomal and genetic defects) and exogenous (unfavorable environmental conditions, inadequate nutrition, stress) factors take part in the development of DST [12, 30, 43]. The peculiarity of connective tissue morphogenesis is that it participates in the formation of the heart frame at almost all stages of ontogenesis; therefore, the influence of any damaging factor can lead to the development of cardiac dystrophy [15].
In 1990, in the classification of diseases of the cardiovascular system of the New York Association of Cardiologists, as well as in Omsk, at a symposium dedicated to the problem of connective tissue dysplasia, the syndrome of cardiac dysplasia, accompanying both differentiated and undifferentiated dysplasia, was first identified. In case of DST syndrome of the heart, its connective tissue framework is involved in the pathological process - heart valves (atrioventricular, semilunar, Eustachian valve), subvalvular apparatus, heart septa and great vessels.
In clinical practice, when it comes to the morphological basis of changes in the cardiovascular system without hemodynamic disturbances, Yu. M. Belozerov (1993) and S. F. Gnusaev (1995) instead of the term “DST of the heart” proposed another one - “minor developmental anomalies heart" (MARS) [3, 8]. According to the definition of these authors, MARS are considered anatomical changes in the architecture of the heart and great vessels that do not lead to gross impairment of the functions of the cardiovascular system [9].
Classification of MARS according to S. F. Gnusaev, 2001 (as amended)
- Localization and form:
atria and interatrial septum: prolapsed valve of the inferior vena cava, enlarged Eustachian valve more than 1 cm, patent foramen ovale, small aneurysm of the interatrial septum, prolapsed pectineus muscles in the right atrium;tricuspid valve: displacement of the septal leaflet into the cavity of the right ventricle within 10 mm, dilatation of the right atrioventricular orifice, prolapse of the tricuspid valve;
pulmonary artery: dilatation of the pulmonary artery trunk, prolapse of the leaflets;
aorta: borderline narrow and wide aortic root, dilatation of the sinus of Valsalva, bicuspid aortic valve, asymmetry and prolapse of the aortic valve leaflets;
left ventricle: trabeculae (transverse, longitudinal, diagonal), small aneurysm of the interventricular septum;
mitral valve: mitral valve prolapse, ectopic attachment of chords, impaired distribution of chords of the anterior and (or) posterior leaflet, “fluttering” chords, additional and abnormally located papillary muscles.
- Complications and associated changes: infectious carditis, calcification, myxomatosis, fibrosis of valve leaflets, chordae ruptures, cardiac arrhythmias.
- Characteristics of hemodynamics: regurgitation, its degree, presence of circulatory failure, pulmonary hypertension.
There is still no consensus on the clinical significance of MARS, many of which are unstable due to the growth of the child. Thus, it is possible to reverse the development of an enlarged Eustachian valve, prolapsed pectineus muscles in the right atrium, mitral valve prolapse (MVP), closure of the open oval window, normalization of the length of the mitral valve chords and the diameter of the great vessels. In some cases, MARS change not only qualitatively, but also quantitatively [3]. Exceeding the established threshold level of cardiac stigmatization in healthy children (more than 3 MARS), according to S. F. Gnusaev (1995), indicates possible disadvantage both in relation to factors influencing the formation of health and indicators characterizing it [8].
Considering that MARS are a variant of visceral DST, children, as a rule, have a pronounced polymorphism of clinical and morphological disorders, depending on the degree of DST and the involvement of other organs and systems in the pathological process. An associative relationship has been identified between the number of external phenotypic markers of CTD and MARS [12, 16, 21, 22]. In this case, not only the number of external phenotypic markers matters, but also the “diagnostic weight” of each of them. It has been noted that skin and skeletal dysplasias are most often combined with MARS [12].
The clinical significance of connective tissue pathology in people with CTD is confirmed by data on the high frequency of neurovegetative disorders, changes in the central nervous system (enuresis, speech defects, vegetative-vascular dystonia (VSD)), and mental disorders [5, 12, 24]. As a rule, VSD is always detected in such patients, which is probably due to hereditary (hereditary) features of the structure and function of the limbic-reticular complex, which determine the abnormal nature of neurovegetative reactions [12]. E. V. Bulankina (2002) established a clear relationship between autonomic dysfunction and DST [4]. At the same time, the severity of dysplastic changes was combined with the severity of the processes of maladaptation of regulatory mechanisms and a decrease in the stress resistance of the body. The most common manifestations of autonomic dysfunction are cephalgia, autonomic crises, vegetative visceral paroxysms, pre- and syncope [12, 16]. According to the data of S.F. Gnusaev (1995), insufficiency of segmental autonomic structures was revealed in persons with MVP [8]. Research by T. M. Domnitskaya (2000) made it possible to establish a direct relationship between MVP, abnormally located trabeculae (ART) and the prevalence of neurotic (neurotic reactions, obsessive-compulsive neurosis, panic disorders) and encephalopathic (cerebrasthenic syndrome, stuttering, tics, sleep disorders, enuresis , hyperdynamic syndrome, fears) disorders [10].
MARS is often accompanied by pathological conditions such as cardiac rhythm and conduction disorders, including early repolarization syndrome, sick sinus syndrome, Wolff–Parkinson–White syndrome, increased electrical activity of the left ventricle, right bundle branch block, extrasystole and paroxysmal tachycardia [ 4, 6, 8, 34]. According to L.A. Balykova et al. (2002), in 90% of patients with cardiac arrhythmias, MARS (mainly MVP) were identified using echography [2]. However, not all MARS are accompanied by heart rhythm disturbances and/or may be their cause. Arrhythmogenic MARS include fibromuscular abnormal chordae (APC) and ART, MVP and tricuspid valve prolapse (TVP), atrial septal aneurysm, enlarged and/or prolapsed Eustachian valve.
The presence of conducting cardiomyocytes in the fibromuscular ARH and ART forms additional conducting pathways, which explains the origin of the impulse that advances intraventricular conduction and causes early excitation of adjacent segments with subsequent earlier repolarization [12, 15, 19, 20, 28]. There is histological confirmation of the presence of conducting cells in the ART with diagonal-basal, mid-transverse and longitudinal localization and in the ART connecting the basal septal sections and the lateral wall of the left ventricle [3, 10, 33]. M. Suwa et al. (1986) noted an increase in the frequency of ventricular extrasystoles with increasing chord thickness. According to E. Chesler et al. (1983), the appearance of ventricular extrasystoles is associated with myxomatous changes in the chordae, causing mechanical irritation of the wall of the left ventricle [27]. The fact that ARX and ART are arrhythmogenic is also confirmed by the disappearance of extrasystoles in patients in the event of their independent rupture or surgical dissection, or during physical activity, when the degree of their tension decreases [8, 10, 12]. A fairly common cardiac arrhythmia in patients with ARH and ART is early ventricular excitation syndrome [6, 12].
Arrhythmias during MVP and PTC, according to various authors, occur in 15 to 90% of cases [11]. Among the causes of arrhythmias, autonomic dysfunction, mechanical stimulation of the endocardium, interstitial magnesium deficiency, psychological stress and myxomatous degeneration of valve leaflets are considered [3, 10–12, 18, 27, 29, 37, 39]. A direct correlation has been established between the frequency and severity of rhythm disturbances and the depth of MVP [1]. A number of authors believe that the cause of the development of arrhythmias in MVP and PTC may be turbulent flow resulting from regurgitation through the valve ring during ventricular systole, especially in PTC, when mechanical irritation of the sinus node area occurs [3, 8, 23]. Most researchers consider excessive tension of the papillary muscles due to their abnormal traction during prolapse of the leaflets as a possible mechanism for the development of ventricular extrasystoles in MVP [12, 14, 25, 38].
The development of arrhythmias can be provoked by a prolapsed Eustachian valve and an aneurysm of the interatrial septum: the conditions for the occurrence of arrhythmias arise as a result of their hilly movements and their reflex irritation of pacemaker formations in the right atrium [42].
According to studies by O. A. Dianov (1999), heart rhythm disturbances occurred in children with a borderline narrow aorta, in whom supraventricular and ventricular extrasystoles were recorded in 32.4% of cases and ventricular extrasystoles in 10.8%, indicating decompensation of adaptation, especially in conditions physical activity [4].
According to Yu. M. Belozerov, children with MARS are characterized by reduced cardiohemodynamic capabilities and demonstrate poor tolerance to physical activity [3]. According to N.A. Mazur, a connection has been established between MVP and sudden death syndrome in adults. Enough information has been accumulated that children with MARS are at risk for developing infective endocarditis.
Thus, existing research results indicate that MARS in some cases are the basis of cardiovascular pathology in children. At the same time, it would be unjustified to exaggerate their role in functional disorders of the cardiovascular system. Obviously, in each specific case the significance of structural abnormalities of the heart must be considered individually.
The principles of therapy for children with MARS have not yet been fully formulated. However, today we can propose the following tactics for the management of children with MARS:
- Comprehensive health assessment, including various types of examination of children.
- The choice of therapy depends on clinical, electrophysiological and echocardiographic changes.
- The use of drugs aimed at normalizing connective tissue metabolism.
- Determination of adequate physical activity depending on the functional state of the myocardium.
The use of non-drug treatment methods is generally accepted, including: - age-appropriate organization of work and rest;
- maintaining a daily routine;
- rational, balanced nutrition;
- psychotherapy and auto-training;
- water and balneotherapy;
- massage (manual, underwater, etc.);
- physiotherapy (electrophoresis with MgSO4, electrosleep, etc.);
- physical education classes, exercise therapy.
The issue of admission to sports is decided individually. In the presence of MVP, it is necessary to take into account family history (cases of sudden death in relatives), the presence of complaints of palpitations, cardialgia; syncope; changes on the ECG (heart rhythm disturbances, short and long QT syndrome) are the basis for deciding whether sports training is contraindicated. This also applies to the presence of ARCH, ART with early ventricular excitation syndrome, which, being arrhythmogenic MARS, can provoke cardiac arrhythmias in athletes under conditions of physical and psycho-emotional stress.
Drug treatment includes the use of:
- magnesium preparations;
- cardiotrophic therapy (in case of disruption of repolarization processes in the myocardium);
- antibacterial therapy for exacerbation of foci of infection, surgical interventions (prevention of infective endocarditis);
- antiarrhythmic drugs (according to indications, with pure group extrasystole with impaired repolarization processes).
Currently, therapy with magnesium preparations for MARS is approaching pathogenetic. This is due to the fact that magnesium is part of the main substance of connective tissue and is necessary for the proper formation of collagen fibers. Under conditions of magnesium deficiency, the ability of fibroblasts to produce collagen is impaired [29, 31]. In addition, magnesium has a membrane-stabilizing effect, retains potassium inside the cell, and prevents sympathicotonic effects, which makes it possible to use it for the treatment of cardiac arrhythmias [40, 41].
In the works of O. B. Stepura (1999), O. D. Ostroumova et al. (2004) there is information about a significant decrease in the degree of MVP, symptoms of VSD, and the number of ventricular extrasystoles during therapy with magnesium drugs [17, 18].
The following medications may be considered appropriate:
Magnerot containing magnesium salt and orotic acid. The latter not only enhances the reabsorption of Mg in the intestine, but also has an independent metabolic effect. Children are prescribed 500 mg of Magnerot (32.8 mg of magnesium 3 times a day for 1 week, then 250 mg 3 times a day for the next 5 weeks. The drug is taken 1 hour before meals).
Magne B6. Available in tablets (48 mg magnesium or in oral solution (100 mg magnesium). Children weighing more than 10 kg (over 1 year) - 5-10 mg/kg/day in 2-3 doses. Children over 12 years old — 3–4 tablets per day, in 2–3 doses, course duration 6–8 weeks.
Potassium orotate. For children, the drug is prescribed at a rate of 10–20 mg/kg/day in 2–3 doses, 1 hour before meals or 4 hours after meals. Course duration - 1 month.
Repeated courses of therapy with these drugs should be carried out (3-4 times a year).
To improve the cellular energy of the myocardium, drugs are used that have a complex effect on metabolic processes in the body, and are also active antioxidants and membrane stabilizers:
- L-carnitine (elkar - 20% solution of carnitine hydrochloride). Doses: 1–6 years, 0.1 g/day (14 drops) 3 times a day; 6–12 years – 0.2–0.3 g/day (1/4 tsp) 3 times a day. Course - 1–1.5 months.
- Coenzyme Q10 (ubiquinone) is prescribed to children over 12 years of age, 1 capsule (500 mg) 1–2 times a day. Preparations containing ubiquinone include kudesan: 1 drop per year of life (up to 12 years), then 12 drops 1 time per day. The duration of the course must be at least 1 month.
- Cytochrome C (cyto-mac). Available in ampoules (4 ml = 15 mg). Prescribed intramuscularly, 4 ml, No. 10. 2–4 courses are given per year.
In addition to these drugs, to improve metabolic processes in connective tissue, myocardium and the body as a whole, the use of:
- nicotinamide (vitamin PP) - 20 mg/day for 1.5–2 months;
- riboflavin (vitamin B2) - 10–15 mg/day for 1.5–2 months;
- thiamine (vitamin B1) - 10 mg/day and lipoic acid 100–500 mg/day for 1.5 months;
- limontara (complex of citric and succinic acid) 5 mg/kg/day 3–4 days weekly for 2 months;
- biotin - 2-5 mg/day - 1.5-2 months.
Repeated courses of treatment are indicated (up to 3 times a year).
In the presence of VSD, complex long-term therapy is carried out to restore the balance between the sympathetic and parasympathetic parts of the autonomic nervous system (differentiated herbal medicine, vegetotropic drugs, nootropics, vasoactive drugs - Cavinton, Vasobral, Instenon, cinnarizine, etc.).
Thus, all of the above allows us to conclude that MARS, being a visceral manifestation of connective tissue dysplasia, constitute the morphological basis of functional changes in cardiac activity and neurovegetative disorders. Choosing an individual course of treatment program helps improve metabolic processes in connective tissue and prevents possible complications of CTD in children and adolescents.
For questions regarding literature, please contact the editor.
N. A. Korovina , Doctor of Medical Sciences, Professor A. A. Tarasova, Candidate of Medical Sciences, Associate Professor T. M. Tvorogova, Candidate of Medical Sciences, Associate Professor L. P. Gavryushova, Candidate of Medical Sciences, Associate Professor M. S. Dzis RMAPO , Moscow
Symptoms

A pediatrician may suspect a disease in a child during a routine examination and examination of the child, paying attention to a systolic murmur during cardiac auscultation.
In most cases, the additional chord of the left ventricle does not bear any functional load on the heart and does not interfere with its normal functioning. For many years, this minor anomaly may not be detected, because it is not accompanied by any special symptoms. A pediatrician can listen to a systolic heart murmur in a newborn, which is detected between the third and fourth ribs to the left of the sternum and does not in any way affect the functioning of the heart.
During intensive development, when the rapid growth of the musculoskeletal system significantly outstrips the growth rate of internal organs, the load on the heart increases, and the additional chord may make itself felt for the first time. Your child may experience the following symptoms:
- dizziness;
- rapid or unmotivated fatigue;
- psycho-emotional lability;
- cardiopalmus;
- pain in the heart area;
- heart rhythm disturbances.
The same clinical manifestations can be observed with multiple abnormal chords of the left ventricle. Most often, such symptoms appear during adolescence. In the future, they can completely disappear on their own, but sometimes they remain in adulthood.
When symptoms appear, the child is required to undergo ECHO-CG, ECG and 24-hour Holter monitoring. These studies will allow the doctor to determine the presence or absence of hemodynamic disturbances. If the additional chord is “hemodynamically insignificant,” then the anomaly is considered safe, and the child only requires follow-up with a cardiologist. With a “hemodynamically significant” diagnosis, the patient is advised to observe, adhere to certain restrictions and, if necessary, treatment.
Signs of an anomaly
If we are talking about a single additional chord in the cavity of the left ventricle (which is the majority), then it may not manifest its existence at all. The doctor may suspect it while listening to the work of the entire organ by the presence of systolic murmur (it should not be present in a healthy organ).
In some cases, during the period of active growth of the child, when the internal organs develop more slowly than the musculoskeletal system, and due to this they receive a more intense load, pain in the cardiac region, dizziness, and increased fatigue may appear.
Another indicator of the presence of an anomaly is arrhythmia.
Attention! With numerous additional chords of the ventricle, there is a possibility of such anomalies in the tissues of other organs, therefore, clinical manifestations may also occur on their part.
Calculate the cost of treatment
Is the accessory chord of the left ventricle dangerous?
Most cardiologists equate such a minor cardiac anomaly with a variant of the norm. The news of the presence of an additional chord in the left ventricle should not cause panic in the child’s parents, since this anomaly does not require surgical treatment and, in the absence of hemodynamic disturbances, does not require drug correction.
In some cases, the additional chord of the left ventricle may become a factor that contributes to the development of other diseases of the heart and blood vessels (infectious endocarditis, cardiac rhythm and conduction disorders, thrombophlebitis, etc.). It is impossible to predict in advance how likely the development of such pathologies is.
Our capabilities
If atypical ventricular chord is suspected or previously identified, the following examinations are recommended:
- Echocardiography is the most informative method for diagnosing various heart pathologies. During the study, the doctor evaluates the structure and contractility of the myocardium, the functioning of the valves, the movement of blood in the chambers of the heart and other indicators.
- A resting ECG is a basic test for assessing heart rhythm. Does not require special training.
You can undergo all diagnostic tests at any KinderKlinik department with subsequent consultation with a specialist.
Need some advice?
Sign up
Callback form
Application has been sent, we will contact you soon
Observation of a child with an additional chord in the absence of hemodynamic disturbances

The main method for diagnosing the accessory chord of the left ventricle is echocardiography.
If an abnormal chord is detected that is not accompanied by symptoms, no special treatment is required. For such patients, it is enough to be regularly monitored by a cardiologist and undergo a control ECHO-CG once a year.
For children with such a minor heart abnormality, it is recommended:
- observe the work and rest schedule;
- Healthy food;
- engage in physical therapy;
- to harden;
- often be in the fresh air;
- prevent stress;
- ensure proper sleep;
- refuse heavy physical activity;
- do not take medications without doctor’s recommendations;
- make a decision about participating in a particular sport together with your doctor.
Parents of such children are not recommended to protect their child from everything and treat him as a disabled person, since this can significantly affect his further socialization. Communication with friends, visiting kindergarten and school, participating in clubs and feasible sports - all this will help the child adapt normally to society and feel complete.
Symptoms and manifestations
An abnormal chord in the heart does not show any characteristic external signs; its existence may not be known for years. Most often, it is detected only during an ultrasound examination, and the basis for referral for an ultrasound is when the doctor listens to a noise in the area during normal heart function, which should not exist.
For information! Murmurs are acoustic phenomena (whistle, creaking) that appear during contraction of the heart muscle, between beats, and are audible when listening with a stethoscope.
The intensity of the noise depends on the location of the abnormal chord of the left ventricle and on their number (if there is a multiple phenomenon). Also, with multiple anomalies, you can notice some features of the general condition:
- increased fatigue;
- mood swings and instability of psycho-emotional state;
- arrhythmia;
- increased heart rate;
- pain in the chest area.
Get a treatment program
Treatment
If an additional chord is detected, which is accompanied by symptoms or hemodynamic disturbances, in addition to the recommendations described above and more stringent restrictions on physical activity, drug therapy is recommended.
These children may be prescribed the following medications:
- vitamins B1, B2, PP - prescribed to improve myocardial nutrition, taken for a month, the course of treatment is repeated twice a year;
- Magne B6, Magnerot, Potassium orotate, Panangin - are prescribed to improve the conduction of nerve impulses and prevent arrhythmias, drugs are selected depending on age and taken in courses for a month or more;
- L-carnitine, Cytochrome C, Ubiquinone - prescribed to normalize metabolic processes in the heart muscle;
- Nootropil, Piracetam - are prescribed when symptoms of neurocirculatory dystonia appear.
Indications for immediate hospitalization in a cardiology hospital may include the following severe heart rhythm disturbances:
- paroxysmal tachycardia;
- atrial fibrillation;
- Wolff-Parkinson-White syndrome;
- Morgagni-Adams-Stokes syndrome;
- extrasystole.
They can develop with multiple or transverse chordae and require detailed examination and subsequent treatment.
In rare cases, muscle fibers of the cardiac conduction system may be included in the structure of the accessory chord of the left ventricle. Such cardiac abnormalities can cause ventricular arrhythmias and ventricular fibrillation. To eliminate them, the following surgical interventions are indicated:
- cryodestruction;
- excision of the chord.
Diagnostics
Directly at the appointment, the doctor conducts a conversation, visual examination and listens to the heart. Some experts argue that in the presence of an additional chord of the left ventricle, specific murmurs can be heard. However, only ultrasound can give the true picture. Even an experienced doctor must first give a referral for an ultrasound examination, and only based on its results make a diagnosis and prescribe treatment.

Carrying out ultrasound in children has a number of its own characteristics. Only from the age of 6 can one count on the child’s adequate perception of the examination situation. Therefore, one of the parents or close people accompanies the child to the ultrasound. The office must be equipped with toys and take into account the age characteristics of patients. Small children, and especially newborns, should not take off all their clothes; it is enough to expose the chest to access the required area.
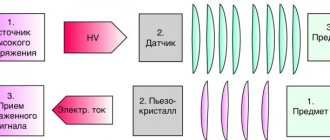
Modern ultrasound examination includes 2 procedures. The first is called echocardiography. With its help, you can examine the structure of the heart with maximum accuracy and characterize hemodynamics. In addition, echocardiography allows you to calculate indicators of most cardiac functions. The second cardiac ultrasound procedure is a Doppler study of intracardiac hemodynamics.
Today, cardiac ultrasound is performed in two-dimensional space, which makes it possible to assess dynamic changes in real time. Ideally, the test is performed with the patient lying on his back. However, in the case of small children, this is difficult to achieve, so you can put the child on his right side, stand him up or sit him down. The main thing is to achieve a calm position, but do not forget about subsequent correction of the results depending on the examination position.
The examination is carried out through the anterior wall of the chest, on the left side of the sternum. In this area the heart is as open as possible. The installation of the sensor depends on the age of the child; the younger it is, the higher the device is installed. In the case of newborns, the sensor can be installed directly on the sternum. To identify an additional chord of the left ventricle, a four-chamber position is usually used, in which abnormal areas appear as linear formations.
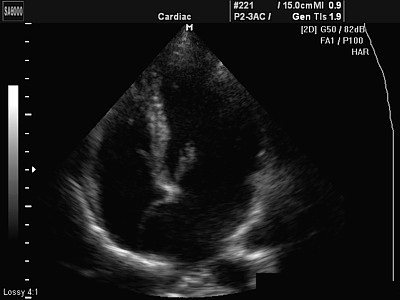
Additional chord, which is visible in the image
The examination procedure, as well as interpretation of the results, takes about 40 minutes. Ultrasound of the heart allows you to assess the condition of the chambers, the size, as well as the integrity of the organ and its structures, the characteristics of blood circulation, the specifics of the pericardial sac and the characteristics of the fluid. All indicators are significant. They may indicate not just the presence of an abnormal appearance of an additional chord, but also concomitant heart diseases.
Prevention
In most cases, an additional chord of the left ventricle appears due to a hereditary predisposition, and it is almost impossible to prevent its development in the prenatal period. Despite this, scientists do not exclude the possibility of the development of such a minor cardiac anomaly under the influence of certain unfavorable factors. That is why pregnant women are recommended:
- Eat properly.
- Stop smoking, drinking alcohol and drugs.
- Avoid heavy physical activity.
- Prevent stress.
- Walk in the fresh air and do gymnastics.
If an additional chord of the left ventricle is detected in a child, parents should pay close attention to his health, follow all the doctor’s recommendations, but not completely protect him from society. An important measure to prevent complications will be the timely treatment of chronic diseases that can be complicated by heart disease.
Children with an additional chord are recommended to regularly engage in physical therapy, which involves individual selection of the load. Wall bars exercises, dancing, gymnastics, sprinting, jumping rope - these activities will help strengthen the heart muscle and prevent the development of complications.
Physical activity should not be excessive, as it can aggravate the situation. Most cardiologists do not recommend that people with accessory chordae engage in professional sports. And such types of stress that occur during diving, snorkeling or parachute jumping are absolutely contraindicated.
Prevention of undesirable consequences
An additional chord in the heart, a photo of which can be viewed today on the Internet resource, regardless of where it is located and what features it has, requires general preventive measures:
- proper distribution of physical activity;
- hardening;
- walks in the fresh air;
- a complete, balanced diet containing the maximum amount of vitamins and beneficial microelements;
- compliance with the daily routine and rest.
The ability to play sports is determined by the attending physician.
For information! Extreme sports and diving are strictly not recommended for anyone who has abnormalities in the heart muscle.
Forecast
In most cases - favorable. Even when symptoms develop, many years pass before the process reaches a critical, decompensated phase.
This can only be achieved consciously. Typically, symptoms in the earlier stages are unbearable and significantly reduce the quality of life. There is no choice but to see a doctor.
The survival rate is good, the likelihood of maintaining working capacity is also good. But this does not mean that you need to sit idly by. You cannot do without the consultation and help of a cardiologist.
Causes of anomalies
An additional chord is formed even before the baby is born, when the formation of the cardiovascular system occurs (“Pregnancy: fetal development and sensations”). The reason for the formation of an additional chord in a child may be:
- heredity - as a rule, this feature is transmitted through the female line;
- improper or insufficient nutrition of the expectant mother;
- nervous tension and stress while expecting a child;
- poor environmental conditions;
- transmission of infectious diseases during pregnancy;
- bad habits during pregnancy (especially in the first trimester).

Smoking and drinking alcohol during pregnancy can lead to abnormalities