Kinds
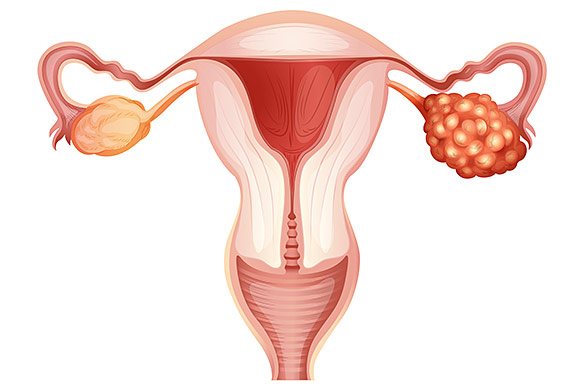
Ovarian oncology can be primary or secondary. In the first case, the tumor develops directly in the gland itself. This disease usually occurs in women under 30 years of age. Secondary cancer, which accounts for up to 80% of cases, arises from various ovarian cysts. It is more often diagnosed in women 50-60 years old - different varieties have their own age limits.
The third option is ovarian cancer, which develops due to metastatic damage to the glands as a result of the development of an oncological tumor in another organ. For example, primary cancer may be in the stomach, breast, uterus, or thyroid gland.
Reviews from our patients
- Chemotherapy - review by Svetlana Vyacheslavovna
Chemotherapy - review by Svetlana Vyacheslavovna May 12, 2021Svetlana Vyacheslavovna arrived at the clinic on the 17th with ovarian cancer, a classic for women, but already with an early pre-treated condition. She was treated and had a long remission. But, based on her general health, she suspected a return of symptoms and contacted our clinic. After further examination, unfortunately, the progression of the disease was discovered. We held a consultation and decided to start...
read more
- Treatment of ovarian cancer. Patient's review
Treatment of ovarian cancer. Patient review January 15, 2021
The patient came to the Medicine 24/7 clinic due to ovarian disease. A comprehensive examination was carried out. Its results were discussed at a medical council. A decision was made to perform an operation involving extirpation of the uterus and appendages, removal of regional lymph nodes, as well as intra-abdominal hyperthermic chemotherapy (HIPEC). The surgery was successful. On the seventh day the patient was discharged in satisfactory condition...
read more
- Treatment of recurrent ovarian cancer. Patient's review
Treatment of recurrent ovarian cancer. Patient review January 14, 2021
The patient was admitted to the Medicine 24/7 clinic with progressive ovarian disease. Before this, surgery and chemotherapy courses were performed. A comprehensive examination was carried out. Its results were discussed at a medical council. The decision was made to carry out the operation. The surgery was successful. On the sixth day the patient was discharged home in satisfactory condition. In the future, chemotherapy courses are planned to minimize the risk of relapse.
read more
- Feedback on treatment for cancer recurrence
Cancer Recurrence Treatment Review November 20, 2021
The patient presented due to relapse of ovarian cancer. The treatment options offered in other clinics did not suit her due to their ineffectiveness. The medical council decided to perform a surgical operation. The recurrent tumor and regional lymph nodes were removed. To prevent further relapses, a HIPEC procedure was performed. The rehabilitation period passed without complications. The patient was discharged home on the ninth day after surgery. Further…
read more
- Feedback on the treatment of stage IV ovarian cancer 10/08/2020
Feedback on the treatment of stage IV ovarian cancer 10/08/2020 October 8, 2021
The patient is aged 75 years. Diagnosis: stage IV ovarian cancer, ascites. The purpose of hospitalization is diagnosis and development of a comprehensive treatment plan. The examination allowed us to verify the tumor and begin chemotherapy courses. The patient tolerated the first one well, all side effects were stopped, there were no complications.
read more
- Feedback on the treatment of stage IV ovarian cancer 08/19/2020
Feedback on the treatment of stage IV ovarian cancer 08/19/2020 August 19, 2021
The patient was admitted in serious condition. She couldn't walk. Diagnosis: stage IV ovarian cancer with metastases, ascites. Other medical institutions refused treatment. The patient underwent laparocentesis. Ascitic fluid is removed through a small puncture in the abdominal wall. A course of chemotherapy was carried out. The patient's condition is stabilized. Thanks to the assistance provided, the patient leaves the Medicine 24/7 clinic feeling well on her feet. “I’m leaving on my own two feet….
read more
- "Thank you for life!" — review from a patient at the Medicine 24/7 clinic
"Thank you for life!" — review from a patient at the Medicine 24/7 clinic August 21, 2021
Olga Vyacheslavovna arrived at the clinic in extremely serious condition. Upon admission, the doctor diagnosed the patient with dehydration, exhaustion, cholemia, peritoneal carcinomatosis and ascites due to ovarian cancer. For almost two weeks, clinic doctors struggled with severe symptoms of the disease. At the time of discharge, Olga Vyacheslavovna’s condition was stabilized. The patient can move independently and eat. Olga Vyacheslavovna plans to undergo further treatment of the underlying disease…
read more
Symptoms
Since the symptoms of an ovarian tumor are nonspecific, at first the problem does not manifest itself in any way, and then begins to disguise itself as other diseases - for example, diseases of the bladder or intestines. The disease also progresses gradually.
Among the possible (but optional) symptoms of ovarian cancer in women, we highlight:
- Feeling of heaviness in the stomach, indigestion. Increased gas formation, bloating, and nausea may occur.
- Changes in bowel habits that cannot be explained by eating a particular food. Alternating constipation and diarrhea.
- Strong and sudden urge to urinate
- Soreness, discomfort in the lower abdomen.
- Weight loss or gain for no apparent reason, problems with appetite. Increase in waist size.
- Pain during sexual intercourse, as well as lumbar pain.
- Weakness, fatigue, lethargy.
A huge problem is that due to the variety of early signs of ovarian cancer, doctors are not always able to make an accurate diagnosis quickly. Usually this is done in three months, but sometimes it takes six months or even more to solve such a problem. And delay in treating such a disease is extremely dangerous.
Survival prognosis
The 5-year survival prognosis (% of patients alive 5 years after diagnosis) for ovarian cancer depends on how far the tumor tissue has spread in the body:
- If the malignant tumor is located only within the ovary: 93–98%.
- If the malignant tumor has spread to neighboring organs and/or regional lymph nodes: 75–94%.
- If there are distant metastases: 31–73%.
Since there are often no symptoms in the early stages, many women are diagnosed with ovarian cancer when the malignant tumor has already spread to other organs. However, even such malignant tumors can often be successfully combated. The Medicine 24/7 clinic uses the most modern techniques for this.
The material was prepared by gynecologist, oncologist at the Medicine 24/7 clinic, candidate of medical sciences Alimardonov Murad Bekmurotovich.
Causes and risk factors
Risk factors for ovarian cancer include:
- Late labor or absence of childbirth in a woman.
- Illiterately selected OK. The same applies to cases when oral contraceptives are selected correctly, but are used for other purposes.
- Menopause.
- Age 45-50 years.
- Long-term treatment for infertility.
- Some gynecological diseases - cysts, fibroids, etc.
- Bad heredity.
- Bad habits.
- Severe weakening of the immune system for various reasons - physical, stress, etc.
Women who have several such factors should monitor their health even more closely.
Diagnostics
Suspicion of ovarian cancer requires a comprehensive comprehensive diagnosis, which includes the following:
- Examination by a gynecologist, colposcopy, palpation of the abdomen, rectovaginal examination.
- Transvaginal ultrasound, CT and MRI of the pelvis.
- Laparoscopy for diagnostic purposes. It is needed to do a biopsy - to take a piece of the tumor for laboratory testing, as well as materials for a number of other tests.
- Blood test for different types of tumor markers.
- Studies to exclude metastases. This group includes mammography, X-rays of the lungs and stomach, ultrasound of the abdominal and pleural cavity, thyroid gland, FGDS, and various intestinal studies.
Clinical guidelines for ovarian cancer suggest undergoing a large number of procedures - but this is necessary, especially since the disease is often discovered when it is actively developing.
References
- Elattar, A., Bryant, A., Winter-Roach, B. et al. Optimal primary surgical treatment for advanced epithelial ovarian cancer, 2011.
- Clinical laboratory diagnostics. National leadership in two volumes / ed. V.V. Dolgova - M.: GEOTAR-Media, 2012. — 928 p.
- Solopova, A.E., Chashchin, A.A., Solopova, A.G. and others. Epithelial ovarian cancer. Clinical lecture, 2021.
- Solopova, A.E., Chashchin, A.A., Solopova, A.G. and others. Modern views on the pathogenesis and diagnostic capabilities of epithelial ovarian cancer, 201.
- Nemaltsova, E.V., Sukhina, E.N., Sukhin, V.S. Determination of the diagnostic information value of the HE-4 tumor marker depending on the morphological structure of the ovarian tumor, 2021. - T. 6(3).
- Ovarian cancer, fallopian tube cancer, primary peritoneal cancer / Clinical guidelines, 2021. - 32 p.
Treatment

When treating ovarian cancer, several approaches are combined:
- Surgical treatment. It comes in different types and volumes - it all depends on the stage and situation. Most often, the uterus is removed, as well as the fallopian tubes and adjacent ovaries. Often, removal of individual lymph nodes and more extensive interventions are required. In later stages, we are talking about inoperable tumors, so surgery is not performed.
- Polychemotherapy. It is carried out to prepare for surgery, after it, and also as an independent means of treatment if the process has already started and surgery is impossible.
- Radiation therapy. As a rule, it is not used in the treatment of ovarian cancer because it has little effectiveness.
After treatment, patients continue to be monitored by a gynecological oncologist in order to promptly detect relapses, if they occur, and other undesirable conditions.
Forecasts
Taking into account the type of tumor, five-year survival at the first stage is possible for 60-90% of patients, at the second stage - for 40-50%, at the third stage - for 11% and at the fourth stage - only 5%.
Sonographic picture of ovarian cancer
The value of echography for diagnosing ovarian cancer . This is mainly determined by the peculiarities of the clinical course of ovarian cancer, namely the absence of any symptoms in the early stages of the disease, in contrast to other malignant tumors of the female genital organs.
During an ultrasound examination of patients with ovarian cancer, the researcher must answer the following questions:
- the tumor affects one ovary or both;
- is there infiltration of the pelvic peritoneum;
- is there ascites;
- is there metastatic damage to the liver and lymph nodes of the para-aortic region;
- is there any involvement of the greater omentum in the tumor process and dissemination throughout the peritoneum;
- is there fluid in the pleural cavities?
In the structure of malignant neoplasms of the female genital organs, the specific frequency of ovarian cancer is 26.4%. At the same time, ovarian cancer ranks first among the causes of mortality from tumors of the female genital organs.
Currently, the following pathogenetic variants of ovarian cancer : primary, secondary (cancer in a cystoma, cyst) and metastatic. The specific incidence of primary ovarian cancer is no more than 5% of all ovarian tumors.
In primary cancer, the tumor is initially formed from the covering epithelium of the ovary and, therefore, there is no mixture of benign and malignant elements. Secondary cancer (cancer in a cystoma, cyst) is the most common malignant ovarian tumor (80-85% of all forms of ovarian cancer), develops mainly in papillary cystadenomas. Metastatic cancer (Krukenberg tumor) occurs as a result of the spread of malignant cells from the primary site (gastrointestinal tract, mammary glands, lungs, etc.) by hematogenous, lymphogenous or implantation routes. In most cases, the source of Krukenberg metastases are tumors of the gastrointestinal tract (the specific frequency of which reaches 20%).
Depending on the echographic structure, malignant ovarian tumors are divided into four variants: solid, solid-cystic, cystic-solid, cystic. In addition, there are several signs that characterize malignant ovarian tumors: a mixed internal structure, the presence of septations, compactions, blurred contours, and ascites. A solid structure most often has a primary cancer, and a cystic or cystic-solid structure is a secondary one. The echogenicity of the formation can be different: low, medium or high.
Importance should be given to the examination of postmenopausal women. In this category of patients, an essential criterion for diagnosing ovarian cancer is the size of the ovaries: ovaries with an average diameter of 30-40 mm should be regarded as abnormally enlarged. When diagnosing ovarian cancer, special attention should be paid to the internal structure of the formation. A fairly reliable sign of ovarian cancer is the presence in the fluid formation of multiple septa of unequal thickness or the appearance of fragmentary thickenings in them. These thickenings can have a homogeneous solid structure or a “spongy” or “cellular” structure. Another important echographic sign of a malignant process is the identification of dense fragments of irregular shape in the liquid formation; dense inclusions can occupy either a small or a large part of the tumor.
It should be noted that determination of the extent of ovarian cancer spread is not always possible using ultrasound. This is due to the capabilities of the method. However, in most cases, with a targeted examination of the abdominal cavity, pelvic cavity and retroperitoneal space, it is possible to identify signs of the spread of ovarian cancer.
If, during examination of the pelvic organs, the dense component occupies less than 1/3 of the tumor and is not directly adjacent to its walls, then this usually indicates stage I of spread. When the dense component is directly adjacent to the wall of the formation and a vague outline is determined in this area or there is bilateral ovarian damage, stage II can be assumed. In stage III, echography does not reveal clear boundaries between the tumor and the uterus, and often with the bladder. In stage IV of spread, the tumor is a single conglomerate with the uterus, in which other pelvic organs are often indistinguishable.
Sonography is highly accurate in detecting ascites. In contrast to the accumulation of fluid of another origin in the abdominal cavity, intestinal loops, usually freely floating in ascitic fluid, in ovarian cancer stick together in the mesentery and take the form of an “atomic mushroom”.
Carcinomatosis of the greater omentum is not always determined, but only when it is significantly affected. In these cases, the omentum involved in the pathological process is depicted as a large flattened hypoechoic, hyperechoic or mixed structure formation located directly under the anterior abdominal wall. The greater omentum may contain metastatic nodes of various shapes and structures. Against the background of a sufficient amount of free fluid in the abdominal cavity, the omentum (with the patient lying on her back and especially with the patient standing) is clearly contrasted (as if floating in the fluid) behind the anterior abdominal wall. In the absence of ascites, it is possible to visualize damage to the greater omentum if it contains hypoechoic foci. With the isoechoic structure of the omentum and the absence of hypoechoic foci, it is difficult to visualize it, since it is little distinguishable by echogenicity from the tissues of the anterior abdominal wall and adjacent intestinal loops. Therefore, in patients with ovarian cancer in the absence of ascites, a targeted examination of the area of its location (from the greater curvature of the stomach and below to the hypogastric region) using high-frequency sensors for superficial organs is necessary to search for damage to the omentum. In the presence of omental damage, an isoechoic layer of tissue under the anterior abdominal wall moves parallel to the abdominal wall during breathing. Also, small (from 2-3 mm) hypoechoic foci may be visible in the formation, invisible when using standard 3-5 MHz sensors for examining the abdominal cavity.
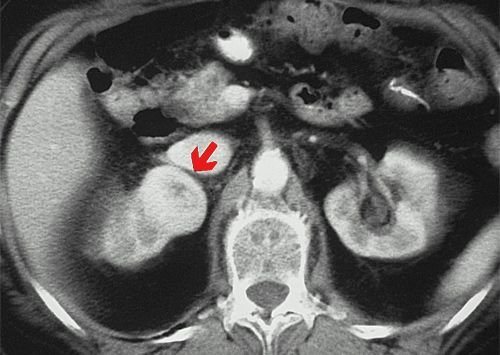
Metastatically affected lymph nodes in ovarian cancer are depicted on scanograms as hypoechoic round or oval formations of various sizes adjacent to the aorta and inferior vena cava, and in later stages - in the supraclavicular areas.
Metastatic ovarian tumors of small sizes (up to 6 cm in diameter), as a rule, repeat the shape of the ovary. New growths that have reached large sizes have an irregular shape, small or coarse contours. The structure of Krukenberg metastases depends on the histological type and location of the primary malignant tumor. In most cases, metastatic ovarian tumors are solid formations, with the exception of metastases from colon and endometrial cancer, which are characterized by a mixed cystic-solid structure. The echographic picture of a typical Krukenberg tumor is distinctive: a solid structure, which is determined by fairly evenly alternating reflections of medium and low echogenicity, with single or round multiple anechoic areas.
As with tumors of other primary locations, ovarian cancer requires examination of the liver to exclude its metastasis.
Also, in case of ovarian cancer, examination of the pleural cavities is necessary, since metastatic pleurisy, both unilateral and bilateral, is characteristic of this disease.
In most cases, ovarian cancer Therefore, ultrasound examination in dynamics, before surgery, provides important information about changes in the size of initially visible nodes, their disappearance or the appearance of new lesions, an increase in the amount of fluid in the peritoneal cavity and in the pleural cavities.
After surgical treatment, ultrasound is one of the leading methods in detecting recurrent ovarian cancer. Local relapse in the pelvic cavity may take the form of a node, infiltrate, free fluid, or a combination of these changes. The smallest dimensions of a recurrent node, visible during ultrasound, are 0.5-0.8 cm. Ultrasound allows one to determine the local extent of a recurrent tumor. Nodules and infiltrates of even small sizes can grow into adjacent organs and structures.
To detect relapse of the tumor process in ovarian cancer, in addition to the pelvic cavity, it is also necessary to examine the following areas:
- abdominal cavity (search for fluid and tumor lesions of the stump of the greater omentum - the area of the omentum in the area of the gastrocolic ligament);
- retroperitoneal space and liver (search for metastases in retroperitoneal lymph nodes and liver);
- soft tissues of the anterior abdominal wall in the area of surgical scars, existing drainages and points of previously performed paracentesis (search for implantation metastases in soft tissues).
In general, the widespread use of ultrasound in gynecological oncology is quite justified; it improves the quality of early diagnosis, reduces the time of examination of gynecological oncological patients, minimizes the use of invasive techniques and expensive radiation examination methods, such as computed tomography and nuclear magnetic resonance imaging.
Prevention
Preventive measures for ovarian cancer include:
- Regular gynecological examination. Once every six months you need to go to an appointment with a gynecologist and treat all detected diseases in a timely manner. Once a year you need to do a gynecological ultrasound.
- Taking oral contraceptives. According to some reports, the risk of ovarian cancer when using them is reduced by 50%. But OCs are selected strictly individually after tests and consultation with an experienced doctor.
- Maintaining a healthy lifestyle, constantly strengthening the immune system.
- Timely examination if even not very obvious symptoms of ovarian cancer are suspected.