- home
- Gynecology
- Adhesions in the pelvis
- Surgery to remove adhesions in the pelvis
Adhesions in the pelvic area are connective tissue strands that appear on the surface of organs, as a result of which the natural mobility of organs is disrupted. The process is accompanied by pain, and serious complications include intestinal obstruction and infertility. Among women visiting the clinic for infertility, in a third of patients the inability to give birth is caused by the presence of adhesions in the pelvic area. In this case, the tubes, ovaries, posterior surface of the uterus, greater omentum, rectum and small intestine may be involved in the process.
In case of pain and the presence of complications, the only effective way to remove adhesions in the pelvis is an operation, the purpose of which is to intersect them and free the organs.
Despite its apparent simplicity, surgery to remove adhesions in the pelvis is a complex intervention that requires the operating surgeon to have extensive experience and the ability to work on adjacent organs located near the uterus. At the stage of planning an operation, it is not always possible to predict the extent of the lesion, the volume and duration of the intervention. Also, at literally every step during the operation, the choice of optimal tactics and the necessary tools is important.
Laparoscopy for fallopian tube pathology
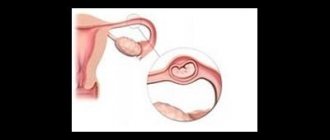
The fallopian tube (fallopian tube) is a paired tubular organ that essentially connects the uterine cavity with the abdominal cavity.
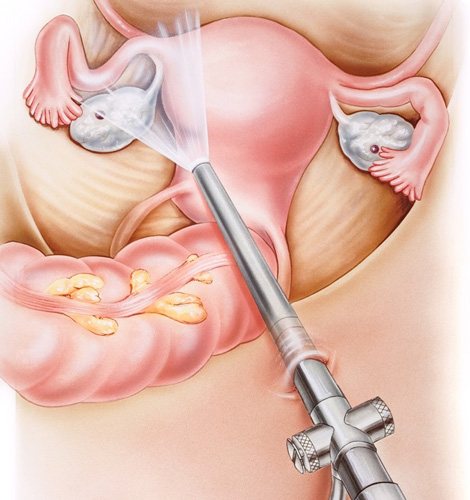
The main function of the fallopian tube is the delivery of a fertilized egg (zygote) to the site of implantation in the endometrium, which is carried out due to the peristalsis of the fallopian tubes and their lining villi towards the uterine cavity. If there are anatomical changes in the fallopian tubes, the entry of the fertilized egg into the uterus is difficult or impossible. Partial obstruction of the fallopian tube, the presence of obstacles in the form of adhesions lead to the “attachment” of the zygote in it and the development of an ectopic pregnancy, which can be accompanied by life-threatening internal bleeding. According to statistics, from 40 to 80% of female infertility is associated with complete obstruction of the fallopian tubes - the so-called tubo-peritoneal infertility. Therefore, one of the important points in examining a woman who has not been pregnant for more than a year is to conduct a diagnostic laparoscopy to assess the patency of the fallopian tubes. This method also makes it possible to cut adhesions and perform tubal plastic surgery, which leads to restoration of their function. In addition, during laparoscopy, other causes of infertility and gynecological diseases are excluded and, if necessary, eliminated.
Laparoscopy is a technique that allows for the diagnosis and treatment of diseases of the abdominal cavity and small pelvis with minimally invasive access through 3-4 incisions on the anterior abdominal wall 5-10 mm long, allowing the installation of special ports in the abdominal cavity. Through them, a laparoscope and instruments are inserted, making it possible to carry out not only a detailed examination of the abdominal and pelvic organs, but also a variety of surgical interventions.
A laparoscope is an optical system consisting of a wide-angle lens, an eyepiece and image transfer sections, which allow not only to transmit an image to the screen, but also to study small objects in detail due to the ability to enlarge the “picture”.
Laparoscopy is divided into two main types - diagnostic and therapeutic. It should be noted that quite often a diagnostic operation is transformed into a therapeutic one if pathological changes were discovered during the examination (for example, benign neoplasms or foci of endometriosis).
The tissue removed during this type of surgery is removed through the same small holes. Since very small incisions are made during laparoscopy, in the postoperative period the pain syndrome is much less pronounced than during an intervention accompanied by a large incision on the anterior abdominal wall.
Patients get up and walk within a few hours after the intervention, and the need for painkillers is reduced. In addition, after laparoscopy, the likelihood of adhesions is lower than after transection.
Indications for the diagnosis and treatment of fallopian tube diseases laparoscopically:
1. Infertility - laparoscopy in combination with chromalpingoscopy - injection of Indigo carmine solution into the uterine cavity and assessment of its entry into the abdominal cavity, allows you to diagnose tubo-peritoneal infertility, detect an obstacle and eliminate it. This method, along with the study of a man’s spermogram, the woman’s hormonal status, and assessment of the presence of ovulation, is one of the main methods for examining an infertile couple. It should be noted that a number of patients are inclined to non-operative methods of studying the patency of the fallopian tubes, such as hysterosalpingography and echosalpingoscopy. However, these methods, in some cases, show false results, so obstruction of the fallopian tubes according to the data is an indication for laparoscopy.
2. An adhesive process after an inflammatory disease of the pelvic organs (adnexitis, salpingoophoritis, peritonitis, etc.), leading to the formation of hydrosalpinx, in which the fallopian tube is closed by adhesions at the ends and fluid accumulates in it.
3. Acute inflammatory process leading to the formation of pyosalpinx (accumulation of pus in the fallopian tube) or tubo-ovarian abscess (purulent melting of ovarian and fallopian tube tissue).
4. Ectopic (tubal) pregnancy - in which the fertilized egg implants in the fallopian tube, growing into its wall, often leading to its rupture and life-threatening internal bleeding.
5. Sterilization - by “ligating” the fallopian tubes. This procedure is performed at the request of a woman over 35 years of age, if she has two or more children, upon the written request of the patient.
Laparoscopy of uterine fibroids
The determining factors when choosing a treatment method for uterine fibroids are the intention to have children in the future, the size of the uterus, the size of the fibroid nodes, and their location. Laparoscopy is a good option for removing small fibroids.
Laparoscopy of uterine fibroids is not performed in the following cases:
- the size of the uterus is larger than the fetus at 11–12 weeks of pregnancy;
- multiple myomatous nodes developed;
- the size of the nodes is large;
- fibroid nodes are located low.
In these cases, it is better to use other removal methods, such as laparotomy.
Contraindications to laparoscopy
Despite a number of advantages and possibilities of laparoscopy, there are absolute and relative contraindications to its implementation. These include:
- state of shock;
- severe infectious diseases;
- bleeding disorders;
- severe diseases of the cardiovascular, respiratory systems, liver, kidneys and other organs in the stage of decompensation;
- large hernia of the anterior abdominal wall;
- infection of the anterior abdominal wall;
- tense ascites;
- pregnancy (second trimester);
- diaphragmatic hernia;
- obesity 3-4 degrees.
Types of laparoscopic operations for tubal pathology.
- diagnostic laparoscopy with chromosalpingoscopy – allows you to assess the patency of the fallopian tubes, identify and remove obstacles;
- salpingoneostomy, fimbryoplasty, fimbryolysis - various types of restoration of patency of the fallopian tube;
- adhesiolysis – separation of adhesions that prevent pregnancy;
- salpingotomy (tubotomy) - dissection of the fallopian tube in order to remove the fertilized egg from it in case of short-term ectopic pregnancy;
- salpingectomy (tubectomy) - removal of the fallopian tube, performed in the presence of hydrosalpinx (an enlarged fallopian tube filled with liquid, the ends of which are sealed on both sides), ectopic pregnancy or pyosalpinx (an enlarged fallopian tube filled with pus);
- resection of part of the fallopian tube - performed for some types of ectopic pregnancy, as well as during sterilization.
GSG, or hysterosalpingography
Hysterosalpingography (HSG) is an X-ray examination of the fallopian tubes for patency. Hysterosalpingography is an important step in the examination of a woman diagnosed with infertility. The accuracy of the study is at least 80%.
Hysterosalpingography allows you to diagnose:
- patency of the fallopian tubes;
- the condition of the uterine cavity and the presence of endometrial pathology - endometrial polyp;
- the presence of developmental deformations of internal organs and the uterus, for example, saddle uterus, intrauterine septum, bicornuate uterus, etc.
Features of the recovery period

Elements of accelerated rehabilitation have been introduced into the work of the gynecological oncology department of UKB 4. One of the aspects of “fact track” surgery is the early activation of the patient, which in such an operation is carried out 5-6 hours after completion of the operation. The patient is allowed to sit down, stand up (the first time under the supervision of medical personnel) and walk if she feels well.
In order to reduce the intensity and relieve pain, intramuscular injections of non-steroidal anti-inflammatory drugs are used, which also contribute to accelerated rehabilitation. Since laparoscopic operations, in comparison with surgical interventions performed by transection, are accompanied by less severe pain, in most cases, the use of narcotic analgesics is not required.
These measures can reduce the risk of postoperative thromboembolic and inflammatory complications, as well as the risk of adhesions.
In addition, all patients are prescribed elastic compression (wearing compression stockings or elastic bandages) to prevent thrombosis of the veins of the lower extremities. Depending on the degree of risk of thromboembolic complications in the postoperative period, low molecular weight heparins or antiplatelet agents may be prescribed, which reduce blood clotting.
As part of rehabilitation therapy, antibacterial drugs are used, as well as agents that normalize intestinal motility and eliminate nausea (if it occurs).
An important point is to follow the correct diet: on the day of the operation, you are not allowed to eat (you can drink still water); for the next 2-3 days, a gentle diet is prescribed until intestinal function is restored.
The following products are not allowed during this period:
- -raw vegetables and fruits;
- -sweets;
- -bakery products;
- -juices, sweet drinks, coffee, carbonated drinks;
- -sweet sour milk products.
If surgical treatment is not associated with an ectopic pregnancy and is not accompanied by intervention on the ovaries (for example, removal of a cyst), menstruation occurs on time (according to the calendar).
However, 1-2 days after chromosalpingoscopy there may be a slight discharge associated with the release of the contrast agent.
The patient spends several days in the hospital (4-6 days), after which she is discharged home (if there are no complications).
It is recommended to limit strenuous physical activity for 21 days after laparoscopy. The duration of sexual rest is determined by the attending physician and depends on the type and extent of the surgical intervention.
In addition, sitz baths, steam baths, saunas, swimming pools, and swimming in the sea are not recommended for about 2 weeks, but the period may vary depending on the extent of the operation and the healing of the sutures.
Sutures are removed 5-7 days after laparoscopy (the day of surgery is not taken into account in the calculation). After this, you can shower completely, including soaking post-operative scars.
At first, the scars are pink in color, then gradually fade and become almost invisible.
Compliance with all doctor’s instructions during the recovery period after laparoscopy helps reduce the likelihood of complications and successful rehabilitation.
Is it worth restoring the patency of the pipes?
You can get pregnant within about a year after the tubes have been restored - the likelihood that they will soon become obstructed again is very high. In addition, the tube must not only be passable: it must transport the fertilized egg to the uterus. If she does not do this, an ectopic pregnancy will form.
Any operation to restore patency of the tubes increases the risk of ectopic pregnancy. Thus, restoring patency is far from a guarantee that you will be able to get pregnant. In addition, any operation can trigger the process of formation of adhesions.
If you are young and there are no more factors that prevent you from getting pregnant, it makes sense to have your tubes operated. If you are over 35 years old and have been trying to have a child for a long time without success, consider artificial insemination. With each ovulation, the “quality” of the eggs deteriorates, and you should not waste months on the restoration of the tubes - time is against you. Based on everything we described above, consult with your doctor to find out whether you should bother with restoring tubal patency at all.
Possible complications after laparoscopy

Surgical interventions performed endoscopically are much easier to tolerate by patients and are less likely to lead to complications compared to conventional operations. Despite this, there is a risk of negative consequences. Any surgical intervention can lead to injury to blood vessels or abdominal organs. This leads to bleeding and inflammatory processes of a purulent nature. Other possible complications include:
- damage to the serous covering of the intestine or bladder;
- accumulation of air in the pleural cavity;
- the occurrence of hematomas.
The possibility of complications associated with anesthesia cannot be excluded. Preparatory measures, including a complete thorough examination of the patient and identification of absolute and relative contraindications, can significantly reduce (and in some cases completely avoid) the occurrence of negative consequences.
Before discharge from the inpatient department, the doctor will set a date for a follow-up examination and/or suture removal. If, after returning home, bleeding from the wound, a strong increase in body temperature, vomiting, accumulation of pus in the area of postoperative wounds and dizziness (up to loss of consciousness) are noticed, it is important to immediately contact a specialist.
Advantages of simultaneous laparoscopy and hysteroscopy
Simultaneous laparoscopy and hysteroscopy operations make it possible to obtain a complete clinical picture in the shortest possible time, which saves patients’ time and effort. The advantages also include:
- low-injury;
- the ability to establish an accurate diagnosis;
- short period of hospitalization;
- fast recovery.
Thanks to the use of modern endoscopic equipment equipped with a video camera, all manipulations are performed with high precision, which eliminates the risk of complications during the procedure.
Why is laparoscopy so popular?
Tubal laparoscopy today is becoming increasingly popular because of its high ability to diagnose a disease located inside a woman’s body and immediately after detection proceed to correcting this pathology. This often makes it possible to avoid open surgery, which is often traumatic.
During tubal laparoscopy, postoperative
the period is much shorter than after traditional surgery.
After this manipulation, the patient’s time in hospital is reduced, and the percentage of adhesions decreases. The procedure is easily tolerated by patients and reduces the cost of treatment. The cost of tubal laparoscopy
is quite affordable for most women.
Laparoscopy has made significant changes to traditional surgery, giving the doctor the opportunity to successfully solve diagnostic problems and, if necessary, treat patients without leaving almost any scars on the body.