Methods for diagnosing gallbladder pathology
Many people underestimate the role of the gallbladder. Some even compare it to the appendix, considering it almost useless. However, it performs a vital function. Its pathologies lead to disruption of the activity of other abdominal organs. To prevent negative consequences, it is necessary to promptly and competently identify dysfunctions. There are many types of gallbladder tests. They are based on five methods:
- The study is carried out using x-rays. A contrast agent is first injected into the organ, which allows you to take a clearer picture.
- Endoscopy provides the opportunity to take a puncture of bile and examine the digestive tract from the inside.
- Ultrasound is the most common method. Primary, on the basis of which additional examinations are prescribed.
- CT – performed using x-rays, but produces a three-dimensional image.
- MRI of the gallbladder is the safest and most informative diagnostic method.
The choice of diagnostic method depends on the suspected disease. However, many of them are quite painful or can cause serious harm to the body due to the use of x-rays. What cannot be said about MRI of the gallbladder and ducts
. Perhaps this is the only way that allows you to examine in detail not only the organ itself, but also its ducts.
What does an MRI of the liver and gallbladder show?
A painless, minimally invasive method for diagnosing gallbladder pathology seemed like a pipe dream ten years ago. The nosology had to be verified using endoscopic cholangiopancreatography. When using this method, a probe had to be inserted into the bile duct through a skin incision. Complications arose after the procedure, and the use was not always rational.
Magnetic resonance imaging reveals a more extensive list of nosological forms and is not characterized by a harmful effect on human health. Timely MRI examination allows you to permanently get rid of the use of invasive endoscopic cholangiopancreatography.
Indications for the use of MRI of the gallbladder and bile ducts
There are a number of symptoms and indications for MRI of the biliary tract and bladder.
Heaviness in the right hypochondrium
It appears in the early stages of gallbladder diseases. May be accompanied by heartburn, bitterness in the mouth, especially after eating fried, fatty, smoked or spicy foods.
Painful sensations in the right hypochondrium
The pain can be of different types. More often these are sharp pains, colic, spasms. They get worse after eating or changing body position, or when bending. More often they indicate difficulty in the outflow of bile or the presence of stones. An MRI of the gallbladder will show what is causing the pain and help determine the general condition of the ducts.
Biliary dyskinesia (BID)
A disease caused by impaired motor function of the bile ducts. This leads to excessive or insufficient flow of bile, which can lead to a number of more serious diseases. MRI of the biliary tract is one of the few methods to recognize this disease.
Stones in the bile ducts (choledocholithiasis) and gallbladder
Poor flow of bile leads to its stagnation. Particles of the thick mass combine with each other, first forming bile sludge, and then their harder form - stones. There are several types of them: cholesterol, pigment, calcareous. Mixed ones are more common. Depending on the composition of the stone and its size, it is possible to remove it non-surgically, but more often operations are performed. The stones are not removed from the gallbladder; they are removed along with the organ. To prevent surgery, it is necessary to perform an MRI of the gallbladder and ducts.
Inflammation of the gallbladder
A disease concomitant with choledocholithiasis. Due to the movement of stones, the walls of the bladder are constantly irritated, thickened and can become inflamed. Also, inflammation of the gallbladder, which is shown on MRI, can occur due to: stress, dietary errors, infection, poor lifestyle, inflammation of other abdominal organs.
MRI of the kidneys, adrenal glands and retroperitoneum
Magnetic resonance imaging (MRI) of the kidneys and MRI of the adrenal glands is an effective diagnostic method and allows high accuracy to differentiate malignant and benign formations of the adrenal glands using special protocols that are highly sensitive to the presence of intracellular fat in adenomas.
Indications for magnetic resonance imaging (MRI) of the kidneys and adrenal glands:
- for injuries,
- patients with contraindications (intolerance to iodine-containing contrast agents for excretory urography);
- to clarify the nature of the space-occupying formation identified using other instrumental research methods (differentiation of normal anatomical structural variants from pathological changes, as well as cysts, from cystic changes in tumor processes in the kidneys);
- patients with clinical data to suspect a kidney tumor,
- if you suspect anomalies in the development of the urinary system,
- in the presence of damage to the retroperitoneal lymph nodes,
- for the diagnosis of perinephric pathological processes,
- changes in perinephric tissue.
MRI of the abdominal cavity and retroperitoneal space - preparation for the study
In order for the abdominal MRI procedure to be most effective, some preparation of the patient is required prior to the examination. The rules are not complicated:
- Examination of the abdominal cavity and retroperitoneal space is carried out on an empty stomach. This is because excess stomach and small intestinal contents reduce image quality and make image reconstruction difficult. The last meal should occur at least 6–8 hours before the test. You should stop drinking 4–6 hours before the start of the study.
- To eliminate increased gas formation, you should take activated carbon before the test (charcoal is taken at the rate of 2 tablets for every 10 kg of body weight). For the same purpose, it is necessary to completely exclude coarse fiber (vegetables and fruits), carbonated drinks, fermented milk products and black bread from the diet the day before diagnosis.
- 30–40 minutes before the test, you need to take 1–2 tablets of an antispasmodic (for example, “No-shpa”).
- Before magnetic resonance imaging of the abdominal cavity, you should not use decorative cosmetics, creams, or hairspray, as this may cause difficulties during the examination.
- A low-carbohydrate diet may be prescribed 2-3 days before an MRI of the pancreas, liver and spleen.
- Immediately before the examination, you must go to the toilet.
In case of emergency, an MRI of the abdominal cavity can be performed without prior preparation.
What diseases can be diagnosed using MRI of the gallbladder?
MRI of the gallbladder and ducts can detect various diseases.
Gallstone disease
This disease is one of the most common. More often it affects women from 20 to 40 years old. The causes that lead to the formation of stones are stress, poor diet, and pregnancy. Stones can be either passive or active - move through the bladder, enter the duct with bile, block it, and cause damage. Gallstone disease is accompanied by pain, heartburn, loss of appetite, and in advanced cases, jaundice. For a detailed examination in this case, MRI of the gallbladder with contrast is used. A contrast agent stains the bile ducts, making them more visible and clear.
Cholecystitis
Inflammatory process in the gallbladder. It can be either acute or chronic. It is often hereditary.
Polyps
Neoplasms on the walls of the gallbladder. The disease is rare compared to others. If the polyps do not cause discomfort to the patient and do not lead to bladder dysfunction, they are not removed.
Dyskinesia
Impaired contractility of the bile ducts. Accompanied by stagnation or excess bile with corresponding symptoms.
How is MR cholangiography done?
At the preparatory stage before the procedure, the patient removes all metal objects. Next, contrast is introduced to improve visualization. The study is performed with the patient in a horizontal position, lying on his back. After this, the table with the patient is placed in the ring part of the magnetic resonance imaging scanner so that it is at the level of the upper abdomen.
During the scanning stage, the ring part of the device rotates around the table. Scanning with a magnetic resonance imaging scanner is accompanied by noise, which can create discomfort for the patient. Therefore, patients undergoing the study are asked to wear earplugs. To obtain accurate and high-quality images, the patient must remain motionless during the entire procedure.
How is the MRI procedure of the gallbladder and its ducts performed?
Before the procedure, many people wonder what an MRI of the gallbladder shows and how it goes.
- First, the doctor finds out whether the patient has contraindications, allergies, phobias or individual reactions. This is especially true for MRI of the gallbladder with contrast.
- Next, the patient changes into loose disposable clothing and removes all metal objects and jewelry.
- The patient lies down on a movable couch, which slides into the tomograph.
- The tomograph scans the affected organ and transfers the results to removable media. It is important to remain still throughout the procedure.
What awaits the patient?
In the modern world, the prognosis for this condition is favorable. This is due to the simplicity of modern diagnosis and well-developed methods of surgical treatment of a disabled gallbladder.
Do not be afraid to remove the organ: it still no longer works and does not bring any benefit. But it does harm, because now it is a source of dangerous inflammation in the body, which it is better to get rid of as soon as possible.
It is believed that postoperative complications are less likely to occur in those patients whose gallbladder has already been disabled for a long time.
An expert on the website Pokhmelye.rf, gastroenterologist Daniela Purgina, dispels a typical myth.
After the bladder is removed, will I have to go on a diet for life? This is not true. You only need to adhere to a diet for the first couple of weeks after cholecystectomy, and then you only need to adhere to the principles of a healthy diet. No strict restrictions are needed.
How to prepare for scanning
Preparation for MRI of the gallbladder includes the following activities:
- A week before the procedure, you must exclude fried foods and fatty foods from the menu.
- Stop consuming dairy products, soda and high-fiber foods within 24 hours.
- The day before the test, take medications that reduce gas formation in the intestines to prevent flatulence.
- On the eve of the examination, do not smoke or drink alcohol.
- The last meal should be no later than 5 hours before the MRI.
- If a child or a person with high nervous excitability is undergoing a scan, it is necessary to take sedatives the day before.
The use of ultrasound and computed tomography in the diagnosis of Klatskin tumor

Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Introduction
Klatskin tumor - extrahepatic cholangiocarcinoma, cholangiocarcinoma of the proximal bile ducts. It accounts for about 10-20% of all neoplasms of the liver ducts, 70-80% of cases of bile duct cancer and about 15% of all malignant liver tumors. In the literature it is also found under the names “portal cholangiocarcinoma”, “hilus tumor”, “portal liver cancer” [2-5, 7, 8].
A primary malignant tumor of the bile ducts was first described by Durand-Fardel in 1840. The term “Klatskin tumor” appeared later when Gerald Klatskin in 1965 reported a tumor (cholangiocarcinoma) arising from the bifurcation of the common hepatic duct.
Bile duct cancer accounts for about 2% of all malignant tumors and is thus the fifth most common malignant tumor of the gastrointestinal tract [1-3, 5, 6, 9].
Cholangiocarcinomas are rare tumors. In recent years, there has been an increase in incidence: 3-4 new cases per 100,000 people. Most common in men over 50 years of age. Carcinomas grow rather slowly and do not manifest themselves clinically. Therefore, about half of all patients have regional lymph node metastases at the time of diagnosis, and thus treatment begins at advanced stages. Previously, central cholangiocarcinoma was considered an inoperable tumor; only palliative treatment was carried out. It is only over the past three decades that invasive surgical methods for tumor removal have replaced a purely palliative approach as a potentially radical treatment. However, even today cure is achieved in approximately 30% of all patients. Despite significant progress in the surgical treatment of hilar cholangiocarcinoma, the prognosis of the disease remains unsatisfactory [2, 4, 6-9].
Tumors of the bile duct bifurcation present certain difficulties for surgeons, which is primarily due to the complexity of the operation, as well as the severity of the condition of this category of patients. In such patients, any surgical intervention carries a high operational and anesthetic risk. Even after radical tumor resection, the 5-year survival rate is only 23 to 46%, and only 9 to 34% if the tumor was detected microscopically at the resection margin [1, 3, 5, 7-9].
For a better understanding of the location of the tumor, below is a diagram of the biliary tree (Fig. 1).
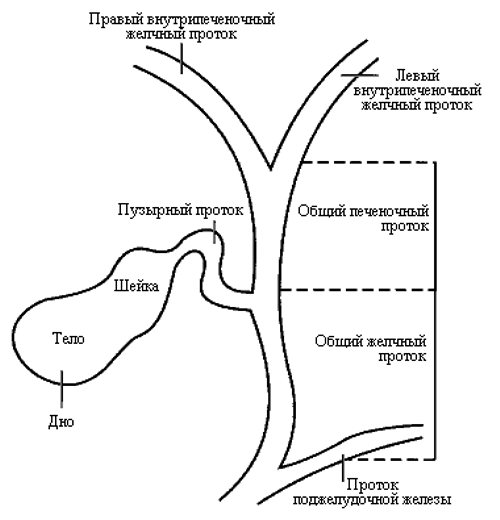
Rice. 1.
Diagram of the biliary tree.
This tumor develops in the upper parts of the bile ducts, in the area of their division between the right and left lobes of the liver. The bile ducts located inside the liver are divided into right and left ducts. A tumor can develop in one of them, or in both of these ducts, in the area where they leave the liver. According to the Bismuth-Corlette classification [9], a distinction is made between tumors that do not reach the bifurcation of the bile ducts (type I) and tumors that extend to the bifurcation (type II). Type III tumor grows through the bifurcation and spreads to the right (type III a) or left (type III b) bile duct. Type IV Klatskin tumor extends from the bifurcation into the left or right bile duct and is a multicentric tumor (Fig. 2). The bile ducts are located next to the blood vessels of the liver, so they are often involved in the process.
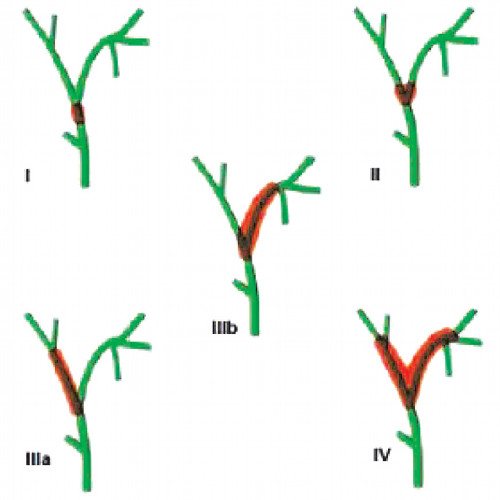
Rice. 2.
Classification of Klatskin tumor according to Bismuth-Corlette.
A distinction is made between tumors that do not reach the bifurcation of the bile ducts (type I) and tumors that extend to the bifurcation (type II). Type III tumor grows through the bifurcation and spreads to the right (type IIIa) or left (type IIIb) bile duct. Type IV Klatskin tumor extends from the bifurcation to the left or right bile duct and is a multicentric tumor.
The clinical picture has all the signs of obstructive jaundice.
Ultrasound examination (US) and computed tomography (CT).
With ultrasound, visualization of the tumor itself is extremely difficult. However, its indirect signs are revealed: the presence of biliary hypertension (high block).
The accuracy of CT is 85-88%, and the detection of obstruction is up to 98.1%. Ultrasound and CT with puncture biopsy increases diagnostic accuracy to 94-96%.
On native CT scans, cholangiocarcinoma appears as a hypodense space-occupying formation with isolated calcifications in it. The expansion of the intrahepatic bile ducts proximal to the tumor location is also determined. After a bolus injection of a contrast agent, a weak peripheral “enhancement” of the tumor and a lack of accumulation of contrast in its central part may occur, even in the late phase. According to other data, after contrasting in the early arterial phase, cholangiocarcinoma quickly and unevenly accumulates the contrast agent over the entire area. Cholangiocarcinoma is characterized by tumor delay of contrast in the delayed phase (hyperdensity), which complicates its differential diagnosis with hemangioma.
The optimal research method for Klatskin tumor can be considered magnetic resonance imaging, which allows not only to determine the precise location of the tumor, but also to visualize in detail the structure of the liver vessels.
With MRI, T2-weighted images are the most informative: on them the tumor gives a relatively high signal intensity, especially in its periphery; areas of low signal in the central part of the tumor appear to correspond to a scar zone. Due to the low vascularity of cholangiocarcinomas, dynamic contrast-enhanced MR imaging is not very effective. In the early, arterial phase of contrast, as with CT, there is an unpronounced peripheral enhancement of the tumor, which in the later, parenchymal phase is replaced by the appearance of a hypointense rim.
As an illustration, we present our own clinical observations.
Clinical observation 1
Patient S., 63 years old, was admitted to the hospital with complaints of yellowing of the skin. She considers herself sick since February 2013, when she began to notice epigastric pain. When jaundice appeared, she was hospitalized in our hospital, where a biochemical blood test revealed: bilirubin 233 µmol/l, direct bilirubin 140.8 µmol/l, indirect bilirubin 92.2 µmol/l, AST 181 U/l, ALT 101 , amylase 25 U/l.
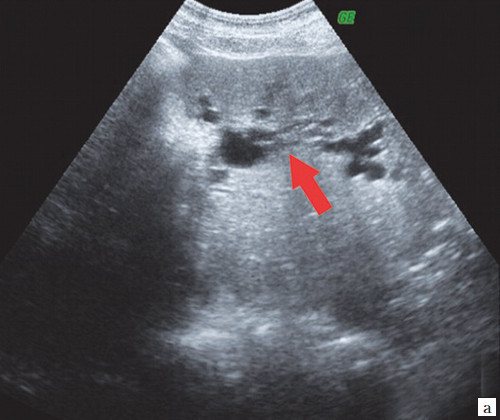
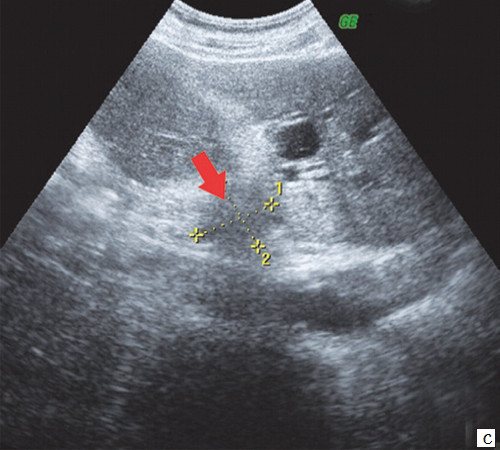
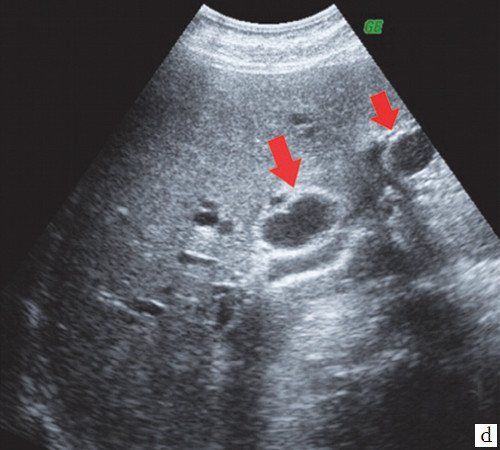
Ultrasound of the abdominal organs: the liver is enlarged in size, the contours are smooth, the echogenicity is increased, the intrahepatic ducts are dilated, lobar up to 7 mm. Portal vein 12 mm. The gallbladder measures 110x38 mm, the wall has a double contour, is completely filled with thick bile, in the projection of the neck there is a fixed calculus up to 14 mm. CBD 6 mm. In the 6th segment of the liver, closely adjacent to the wall of the gallbladder, extending onto the contour of the liver, a liquid formation up to 4 cm in diameter with multiple septations is visualized. The pancreas is of normal size, smooth contours, heterogeneous structure, increased echogenicity, duct 1 mm. The spleen is of normal size and structurally unchanged. Splenic vein 7 mm. Conclusion: Ultrasound signs of biliary hypertension - a high block at the level of the porta hepatis. Gallbladder calculus (wedging of a calculus into the neck of the gallbladder). Ultrasound signs of acute cholecystitis. Paravesical abscess? (Fig. 3).
Rice. 3.
Sonographic picture of patient S.
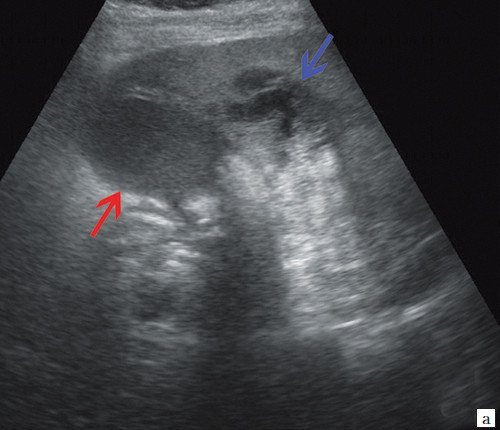
a)
Double contoured gallbladder (red arrow) and paravesical fluid formation (blue arrow).
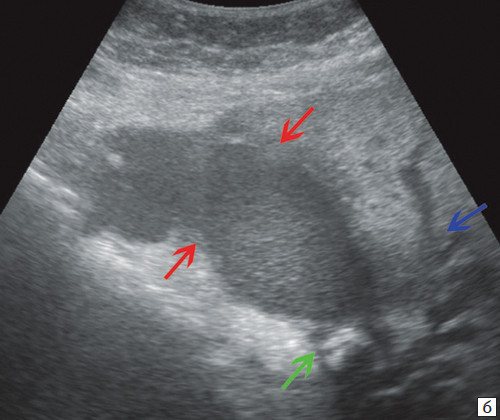
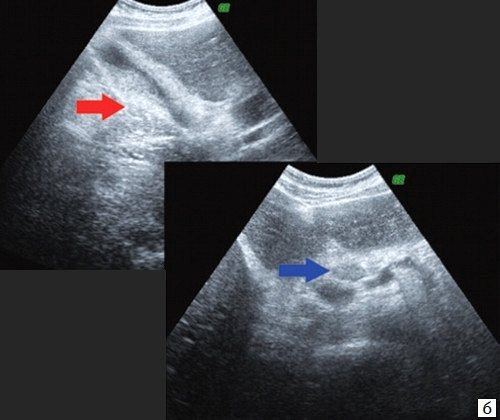
b)
An enlarged gallbladder filled with thick bile (red arrows), a fixed stone in the neck of the gallbladder (green arrow), dilated intrahepatic ducts (blue arrow).
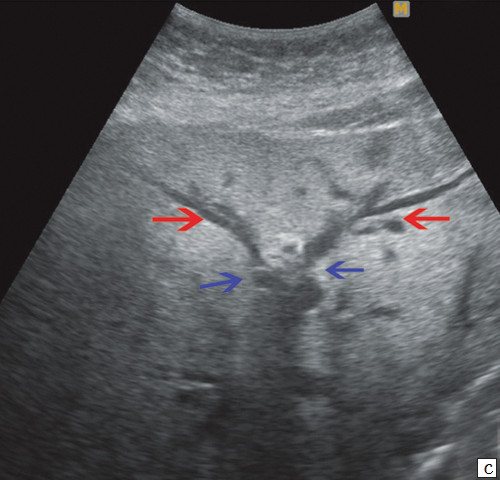
c)
Interruption of duct visualization at the confluence of the lobar ducts of the liver (blue arrows), lobar ducts (red arrows).
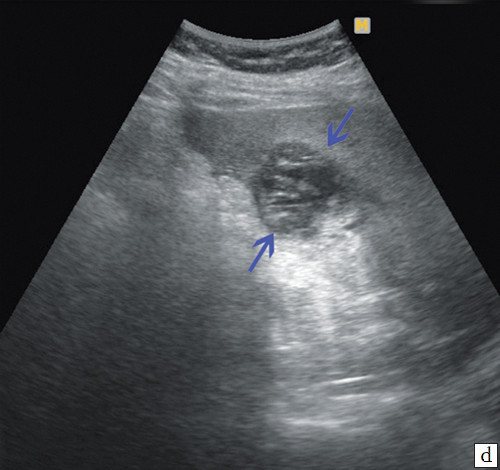
d)
Paravesical formations are liquid in nature, with a large number of septa inside and thick liquid (blue arrows).
According to the MRI conclusion, a gross expansion of the ducts of the right and left lobes of the liver is determined with their break in the projection of the confluence (porta of the liver). The CBD looks normal, no filling defects were found, diameter is 6 mm. The gallbladder contains a large number of small round stones, the contents with a reduced percentage of fluid. The Wirsung duct is 3 mm, not deformed, the contours are even. Conclusion: tumor of the hepatic porta with a separate block (Fig. 4).
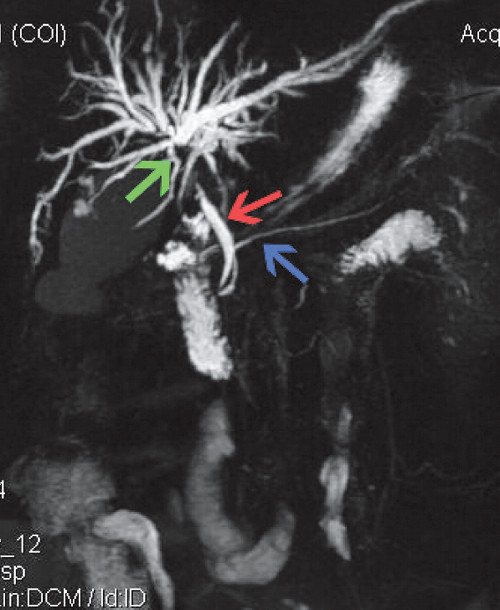
Rice. 4.
MRI for Klatskin tumor. CBD (red arrow), common pancreatic duct (blue arrow), intrahepatic ducts in the bifurcation area (green arrow) - break in the fusion projection.
For therapeutic and diagnostic purposes, a percutaneous transhepatic cholecystostomy was performed, a diagnostic puncture of the paravesical abscess and fistulography were performed.
Under local anesthesia with a 25% solution of novocaine 60.0 ml, a Pigteil 9 Fr drainage was installed into the gallbladder cavity and fixed to the skin with two sutures. About 130 ml of cloudy, dirty gray liquid was removed. The cavity was washed with an aqueous solution of chlorhexidine.
A puncture of the paravesical formation was performed from a separate access, and about 7 ml of turbid bile was obtained.
Fistulography. Water-soluble contrast was introduced through the drainage tube, and the gallbladder measuring 60x30 mm was contrasted. The remaining sections are not contrasted (Fig. 5).

Rice. 5.
Fistulography of patient S. Tumor of the porta hepatis. After percutaneous transhepatic cholecystostomy. Drainage in the gallbladder cavity.
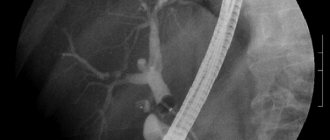
Percutaneous transhepatic cholangiostomy. Puncture of the right segmental duct is impossible due to technical difficulties. Under local anesthesia with a 0.25% novocaine solution, a puncture of the segmental flow of the left lobe of the liver was performed. Cholangiography (Fig. 9) - the ducts of the left lobe are contrasted, the ducts of the right lobe are not contrasted (the block is at the level of the initial section of the left lobar duct). A 9 Fr direct drain is installed along the conductor. When contrast is administered, the ducts of the left lobe of the liver are contrasted. The drainage is fixed to the skin (Fig. 6).
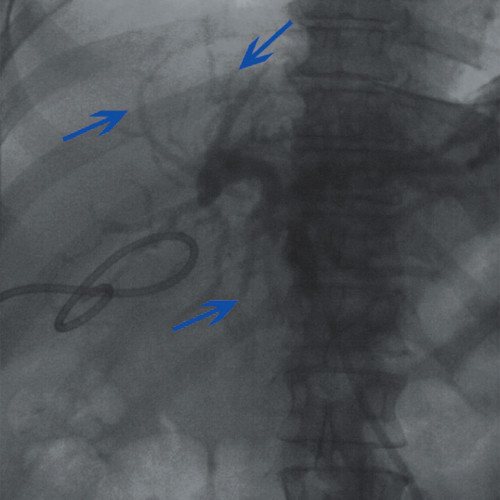
Rice. 6.
Cholangiography of patient S. Tumor of the porta hepatis. Contrasting ducts of the left lobe of the liver (blue arrows).
Ultrasound after installation of cholangiostomy. In the dynamics of free fluid in the abdominal cavity and subdiaphragmatic space on the left. The degree of dilation of the ducts in the left lobe decreased.
Final diagnosis. Tumor of the porta hepatis T4NXMX with a separate block (Klatskin tumor). Mechanical jaundice. GSD acute calculous cholecystitis. Paravesical abscess. Subhepatic infiltrate.
It is impossible to perform a biopsy minimally invasively due to inaccessibility. It is impossible to perform laparotomy due to severe impairment of hemostasis. The patient was discharged for outpatient follow-up treatment.
Clinical observation 2
Patient M., 36 years old, was admitted with complaints of yellowing of the skin without pain and weight loss.
An ultrasound scan of the abdominal cavity revealed that the gallbladder was collapsed and did not contain bile. CBD 6 mm. The pancreas is diffusely heterogeneous, increased echogenicity, duct 1 mm. Signs of intrahepatic hypertension are determined, the right lobar is up to 17 mm, the left lobar is not visualized, the left segmental is up to 10 mm. In the projection of the porta hepatis, a hypoechoic formation 28x26 mm with uneven, indistinct contours is visualized. Enlarged groups inside the abdominal lymph nodes are visualized. Conclusion: Ultrasound picture of a high liver block: Klatskin tumor (Fig. 7).
Rice. 7.
Sonographic picture of patient M.
a)
Dilation of the intrahepatic ducts (arrow).
b)
Collapsed gallbladder (red arrow), paraportal lymph node (blue arrow).
c)
Hypoechoic formation 28 x 26 mm with uneven, indistinct contours at the porta hepatis (arrow).
d)
Enlargement of the right lobar and left segmental ducts (arrows).
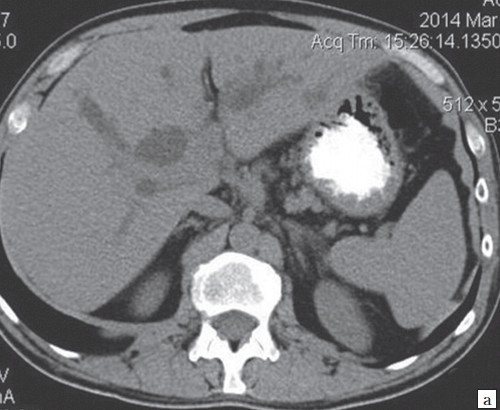
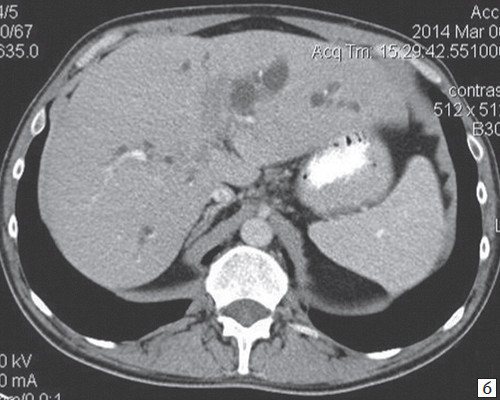
When performing a CT scan of the abdominal cavity at the border of the right and left lobes of the liver, with an irregularly shaped (infiltrative type) formation spreading into the gates of the liver, a formation measuring 25x37x59 mm, unevenly of average intensity, accumulates contrast (CT tumor), at its level the left lobar duct is not visualized and the right one breaks off lobar duct (diameter of the right lobar up to 22 mm). The intrahepatic bile ducts of both lobes are grossly dilated. CBD is not dilated. Lymph nodes of the porta hepatis up to 16 mm. Collapsed gallbladder. The left branch of the portal vein is compressed by the tumor infiltrate. The spleen is of normal shape, not enlarged, the structure and density of the parenchyma is not changed. The pancreas is diffusely heterogeneous, the contours are smooth and clear (Fig. 8).
Rice. 8.
CT scan of the abdominal cavity of patient M.
a)
Native phase.
b)
Arterial phase.
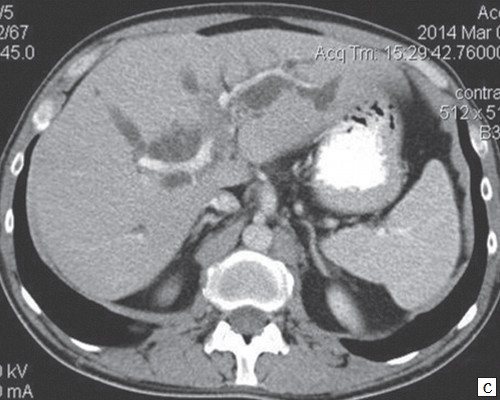
c)
Arterial phase.
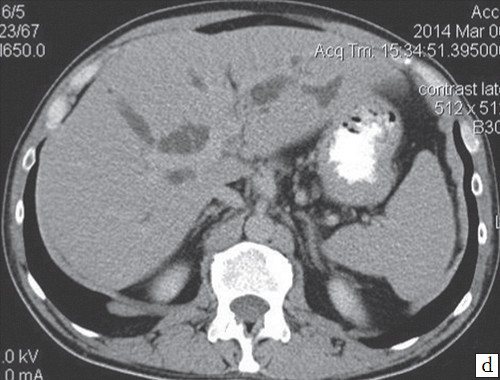
d)
Excretory phase.
Palliative intervention was performed under ultrasound control: two drainages were installed transhepatically in the right and left lobar ducts. The patient has been discharged.
conclusions
Thus, modern diagnostic capabilities using ultrasound, CT and MRI make it possible to clearly establish the localization of the tumor process in the bile ducts and determine the scope of the upcoming intervention.
Literature
- Boyko V.V., Maloshtan A.V. Clinical and anatomical rationale for radical operations for cancer of the extrahepatic bile ducts // Kharkov surgical school - 2008. - N 4(31). — P. 105-113.
- Buryakina S.A., Karmazanovsky G.G. Klatskin tumor: modern aspects of differential diagnosis // Annals of Surgical Hepatology. - 2012. - T. 17. - N 1. - P. 100-109.
- Kozlov A.V., Tarazov P.G., Granov D.A. Methods of interventional radiology in patients with liver and bile duct cancer complicated by obstructive jaundice // Annals of Surgical Hepatology. - 2004. - T. 9. - N 1. - P. 10-19.
- Nazyrov F.G., Ikramov A.I., Akrabov M.M. Diagnosis and tactics of surgical treatment of patients with tumors of the proximal parts of the extrahepatic bile ducts // Surgery. - 2010. - N 6. - P. 36-39.
- Sedov A.P., Parfenov I.P., Mishustin A.M. Klatskin tumor: problems of diagnosis and treatment // Annals of surgical hepatology. - 2006. - T. 11 - N 3. - P. 11-16.
- Ercolani G., Grazi GL, Ravaioli M. Results of surgical treatment for hilar cholangiocarcinoma: a singlecenter experience // HPB. - 2004. - Vol. 6, N 1. - P. 26.
- Harmeet M. Cholangiocarcinoma: modern advances in understanding a deadly old disease // M. Harmeet, J. Gregory // J. Hepatol. - 2006. - Vol. 45, N 6. - R. 856867.
- Kawasaki S., Imamura H., Kobayashi A. Results of surgical resection for patients with hilar bile duct cancer // Ann. Surg. - 2003. - Vol. 238, N 1. - P. 8492.
- Yalcin S. Diagnosis and management of cholangiocarcinomas: a comprehensive review // Hepatogastroenterology. - 2004. - Vol. 51, N 55. - P. 4350.
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.