1.What is blood transfusion and when is it necessary?
A blood transfusion is a medical operation in which blood lost during surgery, injury or illness is replaced with donor blood. Blood is transferred from a special container into your vein through a catheter.
When is a blood transfusion required?
Blood transfusion may be needed in the following cases:
- Blood loss from injury or major surgery;
- Blood loss caused by illness - for example, a bleeding ulcer;
- Diseases that affect blood cells (hemolytic anemia or thrombocytopenia);
- Diseases of the bone marrow - one of the main hematopoietic organs.
A must read! Help with treatment and hospitalization!
Consequences
Complications are divided into early and late. The early ones include:
- Increased body temperature . The reason for this reaction is the breakdown of plasma proteins and leukocytes of donor blood, waste products of microorganisms. The temperature may rise slightly, to medium values, or exceed 40 ° C and be accompanied by severe chills, increased heart rate, and shortness of breath.
- Rash . During blood transfusions, the appearance of rashes accompanied by severe itching is not a rare occurrence. To eliminate them, antihistamines are prescribed. After the rash disappears, blood transfusion may be resumed.
- Acute lung injury . It is usually observed within 2-4 hours after the operation. The complication is life-threatening for the patient. To eliminate it, a person must be connected to a ventilator.
- Acute hemolysis . Mainly due to incompatibility between the donor and recipient. The reaction may not be accompanied by severe clinical symptoms. In the vast majority of cases, the complication leads to death.
- Anaphylactic shock . Occurs in the first minutes from the start of the transfusion. The reaction poses a serious threat to the patient's life.
- Bacterial infection of platelets.
- Air embolism . Associated with air entering the vein. Occurs due to a violation of the technique of the procedure. Accompanied by sharp pain behind the sternum, shortness of breath, and a drop in blood pressure. The outcome is usually unfavorable.
- Thromboembolism . It is caused by blockage of blood vessels by a detached blood clot during transfusion or formed in the blood during its storage.
- Massive blood transfusion syndrome . It is observed when a large amount of donor blood enters the bloodstream in a short period of time. It often causes overload of the cardiovascular system and is accompanied by a complex symptom complex.
- Non-immune hemolysis . Associated with the destruction of red blood cells under the influence of external factors even before they enter the bloodstream. The main symptom is the appearance of blood in the urine, accompanied by or without an increase in body temperature.
- Sepsis . It is more often observed during transfusion of one's own blood components.

The later ones include:
- Alloimmunization . It is observed several days and even months after the transfusion. Alloantibodies are formed to antigens present on the cells of the transfused blood.
- Delayed hemolysis . This reaction usually does not require treatment, but subsequently requires more careful selection of donor blood. It can be suspected if there is an unexplained increase in bilirubin, decreased hemoglobin, or the absence of its increase within 5-10 days with proper transfusion of red blood cells.
- Platelet refractoriness . There is no increase in platelets with their regular infusion. The causes can be both immune and non-immune.
- Graft-versus-host disease . The outcome is always unfavorable. To prevent such a reaction, blood is irradiated.
- Immunomodulation . It is assumed that transfusions may have an impact on the patient's immune status. This is evidenced by the high level of infectious complications in surgical patients and earlier relapses of malignant tumors.
- Purpura . Severe thrombocytopenia develops. It is observed mainly in women who are pregnant or have received blood transfusions.
- Hemosiderosis - accumulation of iron . It is observed mainly in patients who have received red blood cell transfusions for a long time. Iron is deposited in various organs, leading to cardiomyopathy, cirrhosis, and diabetes.
- Infectious complications (hepatitis, syphilis, HIV infection, cytomegalovirus).
2.Is blood transfusion safe?
Donated blood is carefully screened, and blood transfusion surgery is generally quite safe. Nowadays, getting a disease due to a blood transfusion is very rare.
Possible problems with blood transfusion:
- Receipt of incompatible donor blood by the recipient. According to statistics, this happens in one case out of 14,000.
- Problems with the immune system during large blood transfusions. This occurs because the immune system has to suppress viruses received from the donor.
- If your blood types match and the donor does not have any viruses, you may still experience a minor allergic reaction after a blood transfusion. Symptoms include fever, shortness of breath, pain, rapid heart rate, low blood pressure, and chills.
Before major surgery, you can also donate your own blood a couple of weeks before surgery. This way you will protect yourself from all side effects.
Visit our General Surgery page
Post-transfusion complications
Acute dilatation of the heart
It develops as a result of too rapid or massive entry of canned blood into the patient’s venous bed.
In this case, the right parts of the heart cannot cope with pumping the entire incoming volume, resulting in stagnation of blood in the right atrium and the vena cava system. Symptoms occur during blood transfusion or closer to its end. This post-transfusion complication is clinically manifested by difficulty breathing, cyanosis, pain in the right hypochondrium and in the heart region, decreased blood pressure, increased central venous pressure, tachyarrhythmia, and asystole.
First aid for acute cardiac enlargement is to immediately stop the blood infusion and perform bloodletting in a volume of 200–300 ml to relieve the pulmonary circulation. The patient is provided with a supply of humidified oxygen, the introduction of cardiac glycosides (corglycone, strophanthin), vasoconstrictors (phenylephrine, norepinephrine), and furosemide.
Embolic syndrome
Air embolism is a consequence of air entering first a peripheral vein and then into the pulmonary artery with blockage of its trunk or branches. This complication is entirely related to a violation of the intravenous infusion technique, and for its development it is enough for 2-3 cm3 of air to enter a peripheral vein. Post-transfusion thromboembolism occurs when blood vessels are blocked by blood clots or venous thrombi.
In typical cases, a pulmonary embolism syndrome develops, accompanied by sharp pain in the chest, severe cough, shortness of breath, cyanosis, rapid thready pulse, drop in blood pressure, anxiety and agitation of the patient. With massive pulmonary embolism, the prognosis is usually unfavorable.
When the small branches of the pulmonary artery are blocked by small blood clots, a pulmonary infarction develops, the signs of which are chest pain, cough with bloody sputum, low-grade or febrile body temperature. X-ray data of the lungs correspond to the picture of focal pneumonia.
At the first signs of thromboembolic post-transfusion complications, you should immediately stop the blood infusion, begin oxygen inhalation, thrombolytic therapy (administration of heparin, fibrinolysin, streptokinase), and, if necessary, resuscitation measures. If drug thrombolysis is ineffective, pulmonary embolectomy is indicated.
Citrate and potassium intoxication
Citrate intoxication is caused by both the direct toxic effect of the preservative - sodium citrate (sodium citrate), and a change in the ratio of potassium and calcium ions in the blood. Sodium citrate binds calcium ions, causing hypocalcemia. Usually occurs at high rates of administration of preserved blood. Manifestations of this post-transfusion complication include arterial hypotension, increased central venous pressure, convulsive muscle twitching, and ECG changes (prolongation of the Q-T interval). With a high level of hypocalcemia, the development of clonic seizures, bradycardia, asystole, and apnea is possible. The infusion of 10% calcium gluconate solution can weaken or eliminate citrate intoxication.
Potassium intoxication can occur with the rapid administration of red blood cells or canned blood stored for more than 14 days. In these transfusion media, potassium levels increase significantly. Typical signs of hyperkalemia are lethargy, drowsiness, bradycardia, and arrhythmia. In severe cases, ventricular fibrillation and cardiac arrest may occur. Treatment of potassium intoxication involves intravenous administration of a solution of gluconate or calcium chloride, the abolition of all potassium-containing and potassium-sparing drugs, intravenous infusions of saline, glucose and insulin.
Blood transfusion shock
The cause of this post-transfusion complication is most often the infusion of blood incompatible with AB0 or Rh factor, leading to the development of acute intravascular hemolysis. There are three degrees of transfusion shock: at stage I. systolic blood pressure decreases to 90 mm Hg. Art.; at stage II - up to 80-70 mm Hg. Art.; III Art. - below 70 mm Hg. Art. In the development of post-transfusion complications, periods are distinguished: transfusion shock itself, acute renal failure and convalescence.
The first period begins either during the transfusion or immediately after it and lasts up to several hours. There is short-term excitement, general anxiety, chest and lower back pain, shortness of breath. Circulatory disorders develop (arterial hypotension, tachycardia, cardiac arrhythmia), facial redness, and marbling of the skin. Signs of acute intravascular hemolysis include hepatomegaly, jaundice, hyperbilirubinemia, and hemoglobinuria. Coagulation disorders include increased bleeding and disseminated intravascular coagulation syndrome.
The period of acute renal failure lasts up to 8-15 days and includes the stages of oliguria (anuria), polyuria and restoration of renal function. At the beginning of the second period, there is a decrease in diuresis, a decrease in the relative density of urine, after which urination may stop completely. Biochemical changes in the blood include an increase in the level of urea, residual nitrogen, bilirubin, and plasma potassium. In severe cases, uremia develops, leading to the death of the patient. In a favorable scenario, diuresis and renal function are restored. During the period of convalescence, the functions of other internal organs, water and electrolyte balance and homeostasis are normalized.
At the first signs of transfusion shock, the transfusion should be stopped while maintaining venous access. Infusion therapy with blood replacement, polyion, alkaline solutions (reopolyglucin, food gelatin, sodium bicarbonate) begins immediately. Antishock therapy itself includes the administration of prednisolone, aminophylline, and furosemide. The use of narcotic analgesics and antihistamines is indicated.
At the same time, drug correction of hemostasis, organ dysfunction (heart, respiratory failure), and symptomatic therapy are carried out. To remove the products of acute intravascular hemolysis, plasmapheresis is used. If there is a tendency to develop uremia, hemodialysis is required.
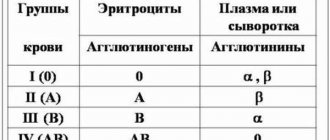
3.What are blood groups and why are they needed?
The AB0 system is the most common blood classification in the world. It is used together with classification by Rh factor. Determining your blood type is very important before any blood transfusion.
Not all blood types are compatible due to antigens.
For example, the first negative blood group is universal donor, because it has no antigens. While the fourth positive, rare blood group is only suitable for transfusion to people with a fourth positive blood group.
About our clinic Chistye Prudy metro station Medintercom page!
How is blood collected for transfusion?
Blood transfusion stations collect blood from willing donors. Any healthy person can come to the blood transfusion station and donate blood. Each donor is selected, and specialists study his medical history to prevent the collection of blood from sick donors.
Donor blood is always carefully checked and its blood type is determined. If there is even the slightest chance that the blood may be unsafe, then it is thrown away.
At blood transfusion stations, blood is also divided into its components, because Sometimes only one component of the blood needs to be transfused.
Blood and its components can be stored and used for a very short time. Therefore, blood transfusion stations always require replenishment.