general description
Systemic lupus erythematosus (SLE) is the most common chronic systemic autoimmune disease belonging to the group of large collagenoses, which is characterized by diffuse damage to connective tissue and blood vessels. Early diagnosis of this pathology is a serious problem, since SLE can begin under the “mask” of other diseases. Since SLE is an autoimmune disease, the mechanism of its clinical manifestations, according to modern concepts, is explained from the following positions:
- circulating immune complexes (CIC), which include antinuclear antibodies, deposited in the microcirculatory link, lead to the development of vasculopathies and tissue damage;
- autoantibodies to blood cells lead to leuko-, lymphothrombopenia and anemia;
- antiphospholipid antibodies lead to the development of antiphospholipid syndrome (APS).
Modern methods of immunological laboratory diagnostics make it possible to identify all components of the pathogenesis of SLE and thereby verify the diagnosis of the disease with extraordinary, almost 100% accuracy. However, the presence of any changes in the analyzes allows them to be interpreted only taking into account the individual clinical picture.
It should be noted that the previous method of diagnosing SLE by the presence of LE cells in the blood did not stand the test of time, showing extremely low sensitivity and specificity, and therefore it was abandoned. LE cells are not even included in the SLE criteria system.
The main markers of SLE are:
- lupus anticoagulant;
- antinuclear factor;
- antibodies to nucleosomes;
- IgG antibodies to double-stranded DNA;
- IgG antibodies to cardiolipin;
- antibodies to cardiolipin class IgM.
Indications for prescribing a blood test for markers of systemic lupus erythematosus
- SLE;
- cutaneous lupus;
- drug-induced lupus;
- rheumatism;
- periarteritis nodosa;
- thrombocytopenic purpura;
- hemolytic anemia;
- pernicious anemia;
- acute leukemia;
- miliary tuberculosis;
- erythroderma;
- severe liver damage;
- plasmacytoma;
- Sjögren's syndrome;
- scleroderma;
- CREST syndrome;
- polymyositis;
- dermatomyositis;
- chronic juvenile arthritis;
- autoimmune hepatitis;
- primary biliary cirrhosis;
- sclerosing cholangitis;
- polyneuropathy;
- myelitis;
- mixed connective tissue disease.
How is the procedure done?
Blood is drawn from the ulnar vein on an empty stomach in the morning.
Preparing for analysis
8 hours before the start of the study, it is recommended to exclude fatty and fried foods, as well as alcohol, from the diet. You are allowed to drink only plain water.
Lupus anticoagulant
Lupus anticoagulants (LA) is one of the important screening and confirmatory tests for diagnosing APS. VAs are formed in the body as a result of the development of autoimmune processes after infectious influences and suppress the reaction of conversion of prothrombin into thrombin in the blood. When these antibodies are detected in the blood by prolongation of coagulation tests, they are defined as “lupus anticoagulant.”
| Normal lupus anticoagulant | |
| negative |
Decoding the analysis result
Positive result:
- SLE;
- APS;
- rheumatoid arthritis;
- ulcerative colitis;
- tumors;
- multiple myeloma.
Antinuclear factor
Antinuclear factor on the HEp-2 cell line (ANF HEp-2, titers; ANA IF, titers). A positive result of ANF is observed in more than 90% of patients with SLE and cutaneous forms of this disease, scleroderma, mixed connective tissue disease, Sjögren's syndrome. The result of determining ANF is the titer, which is the value of the final dilution of the serum at which significant fluorescence of the nucleus remains. The higher the denominator of the fraction, the greater the dilution of the serum, the more antibodies in the patient’s serum. The sensitivity of this test for SLE is 95%.
| Antinuclear factor norm | |
| < 1:160 |
Decoding the analysis result
High ANF titers (1/640 and above):
- high probability of systemic rheumatic disease;
- high probability of autoimmune liver disease;
- an increase in ANF titers over time indicates an exacerbation of a systemic disease;
- in SLE, the titer correlates with the severity of the disease and decreases with effective therapy.
Low ANF titers (up to 1/160):
- in 1-2% of healthy individuals;
- in relatives of patients with systemic diseases;
- many autoimmune, infectious and oncological diseases.
Antibodies to nucleosomes
Nucleosome antibodies (NCAs) are one of the first antibodies to form in the body during the development of SLE. NCA titers correlate with disease activity. The specificity of determining these autoantibodies for diagnosing SLE is more than 95%.
| Norm of antibodies to nucleosomes | |
| < 20 rel. units/ml |
Decoding the analysis result
High levels of antibodies to nucleosomes (positive):
- SLE;
- drug-induced lupus;
- active SLE accompanied by nephritis.
Low levels of antibodies to nucleosomes (negative):
- low probability of SLE;
- low risk of kidney damage in SLE.
IgG antibodies to double-stranded DNA
The presence of IgG antibodies to double-stranded DNA (anti-dsDNA IgG; anti-dsDNA IgG) is highly specific for SLE, and to a lesser extent for other diffuse connective tissue diseases or drug-induced SLE. The sensitivity of the test for SLE is 85%. Quantitative determination of anti-dsDNA IgG antibodies is most suitable for monitoring the condition, prognosis and control of therapy in patients with SLE, as it correlates with its activity and the severity of glomerulonephritis.
| Normal level of IgG antibodies to double-stranded DNA | |
| < 20 IU/ml (negative) ≥ 25 IU/ml (positive) |
Decoding the analysis result
Level up:
- SLE;
- rheumatoid arthritis;
- Sjögren's syndrome;
- scleroderma;
- chronic active hepatitis;
- biliary cirrhosis;
- Epstein-Barr virus infection;
- cytomegalovirus infection.
Downgrade:
- norm.
Anti-cardiolipin IgG antibodies
Anticardiolipin IgG antibodies (aCL IgG) are one of the types of autoimmune antiphospholipid antibodies included in the pathogenesis of antiphospholipid syndrome. Their presence in the blood is manifested by the prolongation of phospholipid-dependent coagulogram tests (prothrombin, aPTT), which is referred to as “lupus anticoagulant”.
| Normal level of antibodies to cardiolipin IgG | |
| <12 GPL-U/ml Negative (no antibodies detected) |
Decoding the analysis result
Positive (antibodies detected):
- APS;
- SLE;
- drug-induced lupus;
- hepatitis C;
- malaria;
- borelliosis;
- syphilis;
- HIV infection.
Antibodies to cardiolipin IgM
Antibodies to cardiolipin IgM (aCL IgM), when detected, indicate a high risk of developing SLE; aCL IgM are detected in 20-50% of patients with systemic lupus erythematosus and 3-20% of patients with other systemic rheumatic diseases.
| Norm of antibodies to cardiolipin IgM | |
| <12 MPL-U/ml Negative (no antibodies detected) |
Interpretation
Positive (antibodies detected):
- APS;
- SLE;
- hepatitis C;
- malaria;
- borelliosis;
- syphilis;
- HIV infection;
- systemic connective tissue diseases.
Systemic lupus erythematosus: caution in dermatologist practice
Summary . Systemic lupus erythematosus (SLE) is an autoimmune disease whose etiology remains unknown. Skin syndrome in SLE is often of paramount diagnostic importance - skin damage in 20-30% of cases is the earliest symptom, and in 60-70% it manifests itself at various stages of the disease, which leads to the patient’s initial visit to a dermatologist. Frequent diagnostic errors are due to the absence of clinical symptoms of systemic damage in the presence of skin manifestations of lupus erythematosus (LE). In this case, laboratory tests are an integral part of the algorithm for managing patients with LE at the stage of contacting a dermatologist. The most specific laboratory test is the determination of antinuclear antibodies using an indirect immunofluorescence reaction, designated as antinuclear factor (ANF). An elevated ANF titer is included in the list of diagnostic criteria for SLE; its detection allows us to assume a diagnosis of SLE and determine a further algorithm for providing medical care. The article presents two clinical cases illustrating abnormalities in immunological tests detected against the background of an isolated skin lesion and the absence of visible somatic pathology. This made it possible to suspect the systemic course of the process at an early stage and refer patients for consultation with a rheumatologist, where the diagnosis of SLE was confirmed.
According to modern concepts, systemic lupus erythematosus (SLE) is an autoimmune disease of unknown etiology, characterized by overproduction of organ-nonspecific autoantibodies with the development of immunoinflammatory damage to the tissues of internal organs [1]. A wide range of autoantibodies produced and their direct or indirect effects on cellular targets determine the variety of clinical manifestations in lupus erythematosus (LE) [2]. SLE can manifest as isolated or combined damage to systems and organs, including damage to the skin and mucous membranes (lupus butterfly, discoid erythema, photosensitivity, alopecia, telangiectasia, livedo reticularis, oral ulcers), the cardiovascular system (pericarditis, myocarditis, endocarditis, coronaritis), kidneys (lupus nephritis), central nervous system (convulsions, psychosis), musculoskeletal system (arthralgia, arthritis), lungs (pleurisy, lupus pneumonitis), hematological disorders (hemolytic anemia, leukopenia, thrombocytopenia), etc. [3].
A key role in the diagnosis of SLE is played by the detection of clinical manifestations of the disease and laboratory diagnostic data [3]. Skin syndrome in SLE is often of paramount diagnostic importance - skin damage in 20-30% of cases is the earliest symptom, and in 60-70% it manifests itself at various stages of the disease, which leads to the patient’s initial visit to a dermatologist [4]. Skin lesions in SLE are polymorphic and are represented by various changes - from minor telangiectasia to bullous lesions [2]. There are lupus-specific and lupus-nonspecific skin lesions, the latter are several times more common. Lupus-specific include various manifestations of chronic, subacute and acute LE [5]. The group of nonspecific lesions includes: photosensitivity, leukocytoclastic and urticarial vasculitis, telangiectasia, livedo reticularis, malignant atrophic papulosis and Raynaud's syndrome [5]. The wide variability of clinical manifestations of the skin syndrome necessitates a careful differential diagnosis [1].
An important tool for the early diagnosis of systemic diseases is the detection of autoantibodies using laboratory tests [3]. The most specific for SLE are antinuclear antibodies (ANA) - this is a heterogeneous group of autoantibodies to components of the cell nucleus, among which are antibodies to double-stranded deoxyribonucleic acid (DNA), histones, nucleosomes, extractable nuclear antigens, nucleolar antigens and other cellular structures [6 ]. The standard method for detecting the ANA group is the indirect immunofluorescence reaction (IDIF) using the human laryngeal adenocarcinoma epithelial cell line (HEp-2) [7]. The determination of ANA by the NRIF method is usually designated as antinuclear factor (ANF), the content of which is assessed by the maximum detected titer in the blood serum, indicating the intensity and type of fluorescence [8]. A quantitative increase in titer over 1:160 is included in the list of diagnostic criteria for SLE according to the recommendations of the American College of Rheumatology (ACR) and the European League Against Rheumatism (ULAR) and is used to assess the activity of the process, prognosis, etc. as a predictor of the development of SLE at the preclinical stage [8].
The long-term formation of the pathognomonic clinical symptom complex of SLE, the lack of necessary laboratory tests and interdisciplinary interaction are the cause of frequent diagnostic errors, leading to the lack of timely anti-inflammatory and immunosuppressive therapy by a rheumatologist. Considering the above, we consider it appropriate to present our own clinical observations.
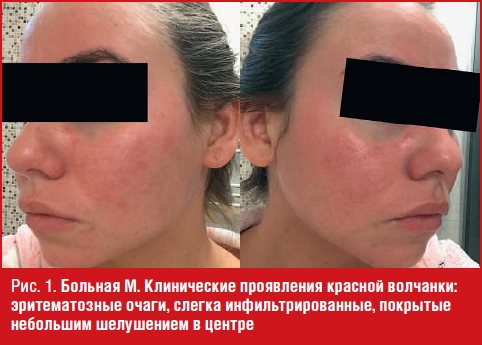
Clinical observation No. 1
Patient M., 27 years old, considers herself sick since July 2021, when after a long vacation on the coast, rashes appeared on the skin of her face. I contacted a dermatologist at my place of residence, where the diagnosis was made: “Rosacea, papulopustular subtype, moderate course.” She received a course of treatment (doxycycline, metronidazole gel). The patient did not notice any visible improvement, the process on the skin continued to progress, and therefore she turned to the Department of Dermatovenereology of the Kuban State Medical University of the Ministry of Health of Russia.
Data from other organs and systems: complains of aching pain in the small joints of the hands and knee joints, a feeling of morning stiffness. Not examined somatically.
Objectively: the skin pathological process is of a limited symmetrical nature, localized on the skin of the wings of the nose, cheeks, and chin. Presented: erythematous spots, scales, telangiectasia.
On the skin of the face (in the area of the wings of the nose, cheeks, chin) there are bright pink erythematous lesions, with clear boundaries, slightly infiltrated, regular round shape, 3-4 cm in diameter, covered with slight peeling in the center of the lesions; Telangiectasias are visualized in the peripheral zone of the lesions (Fig. 1). Removal of scales is accompanied by pain (Besnier-Meshchersky symptom).
The biodose was determined to be 20 seconds.
With a presumptive diagnosis of “Discoid lupus erythematosus?” the patient was sent for histomorphological examination of the skin.
The results of a histomorphological examination of the skin from the pathological lesion on the right cheek: follicular hyperkeratosis; epidermis with a tendency to atrophy; vacuolar degeneration of cells of the basal layer. Under the epidermis, the vessels are dilated. In all parts of the dermis there are dense diffuse and perivascular lymphohistiocytic infiltrates with an admixture of neutrophils and plasma cells. Around the pilosebaceous follicles there is a thick lymphohistiocytic infiltrate with an admixture of neutrophils, mast cells and fibroblasts, penetrating into the outer epithelial vagina. In the dermis there are areas of mucoid swelling of collagen fibers. Conclusion: the morphological picture may correspond to lupus erythematosus.
General clinical examination data: general and biochemical blood tests - indicators are within normal limits; General urinalysis - indicators are within normal limits.
The alarming factors in terms of transformation of the skin form into a systemic process in patient M. were: onset of the disease at a young age, a history of prolonged sun exposure, skin phototype II, biodose of 20 seconds, the presence of severe articular syndrome.
To exclude the diagnosis of SLE, an immunological study was performed:
- Antinuclear factor on HEp-2 cells: 1:320 titer (normal less than 160); fine granular type of glow.
- Antibodies to double-stranded DNA (a-dsDNA) – 53 IU/ml (normal – less than 25 IU/ml).
- Blood test for antibodies to phospholipids of the IgG class (screening) - 10.13 IU/ml (reference values: up to 10 IU/ml - not detected).
- Blood test for antibodies to phospholipids of the IgM class (screening) - 12.68 IU/ml (reference values: up to 10 IU/ml - not detected).
With the obtained data, the patient was referred to a rheumatologist at Regional Clinical Hospital No. 2, where the diagnosis of SLE was confirmed. The patient was registered with a rheumatologist to determine further management and treatment tactics.
Clinical observation No. 2
Patient V., 66 years old, considers herself sick since April 2021, when rashes first appeared on the skin of the cheeks and chin. When collecting anamnesis, it was established that the patient had lived in the northern region for a long time and, after moving to the Krasnodar region, began to notice the appearance of rashes. I used betamethasone and dexpanthenol on my own. She noted a temporary improvement, but in the spring and summer the disease worsened. I contacted a dermatologist at my place of residence, where a diagnosis of “steroid-induced rosacea” was made and treatment was prescribed (topical and systemic antibacterial drugs, angioprotectors). I did not observe any visible improvement, and therefore applied to the Department of Dermatovenereology of the Kuban State Medical University of the Ministry of Health of the Russian Federation.
Objectively: the skin pathological process is widespread, localized on the skin of the face and neck. Presented: spots, telangiectasia, scales.
On the skin of the face in the area of the cheeks, left parotid region and neck there are swollen erythematous foci of a pinkish-red color, 2–3 cm in diameter, predominantly regularly round in shape with slight peeling; single telangiectasias are visualized. Removal of scales is accompanied by pain (Besnier–Meshchersky symptom) (Fig. 2).

With a preliminary diagnosis of “Discoid lupus erythematosus?” The patient was sent for histomorphological examination.
The results of a histomorphological examination of the skin from the pathological focus: on the skin of the left cheek - follicular hyperkeratosis; areas of parakeratosis; the epidermis is atrophic in places; vacuolar degeneration of cells of the basal layer of the epidermis; subepidermal blisters. In the papillary layer there is swelling, the walls of the vessels are thickened. In the dermis there are dense focal and perivascular lymphohistiocytic infiltrates with an admixture of neutrophils. Around the pilosebaceous follicles there is a thick lymphohistiocytic infiltrate with an admixture of neutrophils, mast cells and fibroblasts, penetrating into the outer epithelial vagina. In the dermis there are areas of mucoid swelling of collagen fibers. Conclusion: the morphological picture is more consistent with lupus erythematosus.
General clinical examination data: general and biochemical blood tests revealed the following abnormalities - leukocytes 3.7 × 109/l; cholesterol 8.7 mmol/l.
Considering the duration of the skin pathological process and the lack of examination results from related specialists, an immunological study was performed to exclude the diagnosis of SLE:
- Antinuclear factor on HEp-2 cells: titer 12,560 (normal less than 160); coarse-granular type of glow.
- Antibodies to double-stranded DNA (a-dsDNA) – 0.5 IU/ml (normal – less than 25 IU/ml).
- Blood test for antibodies to phospholipids of the IgG class (screening) 16.65 IU/ml (reference values: up to 10 IU/ml - not detected).
- Blood test for antibodies to phospholipids of the IgM class (screening) - 14.68 IU/ml (reference values up to 10 IU/ml - not detected).
With the results of laboratory tests obtained, the patient was referred for a consultation with a rheumatologist at Regional Clinical Hospital No. 2, where the diagnosis was made: “SLE, chronic course, 1st degree of activity, with skin lesions (butterfly-type erythema), immunological disorders (antinuclear factor on HEp-2 cells, positive blood test for antibodies to phospholipids IgG, IgM).” The patient was hospitalized in the rheumatology department for inpatient treatment.
Discussion
In both patients, against the background of isolated skin lesions and the apparent absence of pathognomonic symptom complexes of SLE, immunological changes were identified, which allowed the dermatologist to suspect the systemic course of the process and refer for consultation to a rheumatologist. Laboratory diagnostics and interdisciplinary interaction made it possible to conduct an early diagnosis of the disease, which, in our opinion, will largely improve the prognosis of the disease and the quality of life of patients.
Thus, immunological studies and their comprehensive analysis are an integral component of the algorithm for managing patients with CV already at the stage of contacting a dermatologist and contribute to the high quality of medical care for this group of patients.
Literature/References
- Tlish M. M., Naatizh Zh. Yu., Sycheva N. L., Kuznetsova T. G., Irizelyan G. A., Psavok F. A. Systemic lupus erythematosus: an interdisciplinary approach to diagnosis // Russian Journal of Skin and Venereal Diseases diseases. 2016; 19 (3): 141-147. Rossiyskiy zhurnal kozhnykh i venericheskikh bolezney. 2016; 19 (3): pp. 141-147.]
- Mazurov V.I., editor. Diffuse connective tissue diseases: a guide for doctors. St. Petersburg: SpetsLit, 2009. 192 p. SPb: SpetsLit, 2009. P. 192.]
- Nasonov E. L., editor. Clinical guidelines for rheumatology. 2nd ed., rev. and additional M.: GEOTARMEDIA, 2010. 429 p. 2-ye izd., ispr. i dop. M.: GEOTARMedia, 2010. P. 429.]
- Romanova N.V., Shilkina N.P. Clinical and immunological characteristics of skin syndrome in patients with lupus erythematosus // Russian Journal of Skin and Venereal Diseases. 2005; (4): 45-48. Rossiyskiy zhurnal kozhnykh i venericheskikh bolezney. 2005; (4): pp. 45-48.]
- Tlish M. M., Naatizh Zh. Yu., Sycheva N. L., Kuznetsova T. G. Systemic lupus erythematosus in the practice of a dermatologist // Clinical Medicine. 2018; 96 (3): 277-281. Klinicheskaya medicsina. 2018; 96(3): pp. 277-281.]
- Klyukvina N. G. Clinical significance of laboratory abnormalities in systemic lupus erythematosus // Modern rheumatology. 2014; (2): 41-47. Modern revmatologiya. 2014; (2): pp. 41-47.]
- Alexandrova E. N., Novikov A. A., Nasonov E. L. Recommendations for laboratory diagnosis of rheumatic diseases of the All-Russian public organization “Association of Rheumatologists of Russia” - 2015 // Modern Rheumatology. 2015; 9 (4): 25-36. Modern revmatologiya. 2015; 9 (4): pp. 25-36.]
- Aleksandrova E. N., Novikov A. A., Verizhnikova Zh. G., Lukina G. V. Modern view on the problems of studying antinuclear antibodies in systemic lupus erythematosus (literature review) // Clinical laboratory diagnostics. 2018; 63 (6): 340-348. Klinicheskaya laboratornaya diagnostika. 2018; 63 (6): pp. 340-348.]
M. M. Tlish, Doctor of Medical Sciences, Professor Zh. Yu. Naatizh1, Candidate of Medical Sciences T. G. Kuznetsova, Candidate of Medical Sciences E. A. Chernenko
Federal State Budgetary Educational Institution of Higher Education Kuban State Medical University of the Ministry of Health of Russia, Krasnodar, Russia
1Contact information
Systemic lupus erythematosus: caution in the practice of a dermatologist / M. M. Tlish, Zh. Yu. Naatizh, T. G. Kuznetsova, E. A. Chernenko For citation: Tlish M. M., Naatizh Zh. Yu., Kuznetsova T. G., Chernenko E. A. Systemic lupus erythematosus: alertness in the practice of a dermatologist // Attending Physician. 2020; vol. 23 (11), 23-26. DOI: 110.26295/OS.2020.35.78.005 Tags: autoimmune disease, skin syndrome, treatment algorithm
Norms
| Index | Norm | |
| Lupus anticoagulant (LA, Lupus anticoagulants, LA) | negated | |
| Antinuclear factor on the HEp-2 cell line (ANF HEp-2, titers; ANA IF, titers) | < 1:160 | |
| Antibodies to nucleosomes | < 20 rel. units/ml | |
| IgG antibodies to double-stranded DNA | <20 IU/ml (negative) | |
| Anticardiolipin IgG antibodies (aCL IgG) | negative or < 12 GPL-units/ml | |
| Anticardiolipin IgM antibodies (aCL IgM) | < 12 MPL-units/ml | |
Causes of SLE
The exact causes of systemic lupus erythematosus are unknown. Lupus is thought to result from a combination of genetic changes and environmental influences. Among the factors that can both provoke SLE and aggravate its course are:
- Smoking.
- Exposure to sunlight.
- Viral diseases.
- Medicines from the groups of antihypertensives, anticonvulsants and antibiotics.
- Childbirth and transition to menopause.
Systemic lupus erythematosus is not a contagious disease and cannot be transmitted from person to person through air, touch, sexual intercourse or any other means except for hereditary tendencies.
Who is at risk?
Risk factors for the development of SLE are:
- Hereditary tendency. People who have blood relatives with SLE may have similar genetic changes that lead to this condition.
- Floor. The vast majority of patients are women.
- Age. Lupus is most often diagnosed between the ages of 15 and 45.
- Race. SLE is more common in African Americans, Hispanics, and Asian Americans.
Diseases for which a doctor may order a blood test for markers of systemic lupus erythematosus
Multiple myeloma
In multiple myeloma, the lupus anticoagulant test is positive.
Syphilis
With syphilis, there is a high concentration of antibodies to cardiolipin IgG, a high concentration of antibodies to cardiolipin IgM.
Ulcerative colitis
In ulcerative colitis, lupus anticoagulant is present in the blood.
Cytomegalovirus infection
With cytomegalovirus infection, a high concentration of IgG antibodies to double-stranded DNA is observed.
Malaria
In malaria, there is a high concentration of antibodies to cardiolipin IgG, a high concentration of antibodies to cardiolipin IgM.
Sjögren's syndrome
In Sjögren's syndrome, there is a high concentration of IgG antibodies to double-stranded DNA.
Systemic lupus erythematosus
With systemic lupus erythematosus, a lupus anticoagulant is present in the blood, high ANF titers (1/640 and above), high levels of antibodies to nucleosomes, high concentrations of IgG antibodies to double-stranded DNA, high concentrations of antibodies to cardiolipin IgG, high concentrations of antibodies to cardiolipin IgG are observed. , high concentration of antibodies to cardiolipin IgM.
Scleroderma
In scleroderma, there is a high concentration of IgG antibodies to double-stranded DNA.
Diagnosis of lupus erythematosus
Because lupus affects multiple organs and symptoms can mimic other diseases, diagnosis is often difficult. However, there is still not a single laboratory test in the world that could definitively confirm the diagnosis.
The diagnosis is based on a combination of symptoms. For correct diagnosis, the doctor uses the following data:
- detailed medical history (patient information);
- detailed medical examination;
- laboratory tests: blood test, sedimentation, biochemical study, urine test, immunological tests - complement level, antinuclear and other autoantibodies;
- imaging methods: x-ray, ultrasound, echocardiography, ultimately magnetic resonance imaging;
- eye examinations;
- neurological examination;
- skin biopsies;
- kidney biopsy, etc.
Laboratory tests of blood and urine
Kidney biopsy
Eye examination
Lupus can cause inflammation of the kidneys (lupus nephritis) and impair the kidneys' ability to eliminate waste products. In this case, blood and protein appear in the urine. If there is a large loss of protein in the urine, the patient may suffer from edema. But in many cases, kidney disease is not accompanied by any symptoms, so urine should be examined in every person with lupus, even those without kidney symptoms.
To diagnose lupus nephritis and determine its type and proper treatment, a sample of kidney tissue is taken (kidney biopsy).
Is lupus dangerous? Complications
Systemic lupus erythematosus is accompanied by damage to a large number of internal organs and systems, leading to numerous complications. The most common lesions of the following organs are:
- Kidneys. As a result of SLE, kidney failure often develops, which is one of the leading causes of death among people with this pathology.
- Brain and central nervous system. As a result of autoimmune damage to the central nervous system, severe headaches, dizziness, cognitive changes, vision problems and even strokes or seizures occur.
- Lungs. SLE is often accompanied by inflammation of the inner lining of the chest, which also covers the lungs - the pleura. Also with this pathology, the development of pulmonary hemorrhages and severe pneumonia is possible.
- Blood and vessels. Lupus can cause problems with your blood system, including a decrease in the number of healthy red blood cells (anemia) and an increased risk of bleeding or clotting. It can also cause inflammation of blood vessels.
- Heart. Lupus can cause inflammation of the heart muscle, arteries, or the lining of the heart (pericardium). Also, with SLE, the risk of cardiovascular diseases and myocardial infarction increases significantly.
Autoimmune disorders that occur in the body with systemic lupus erythematosus can be a trigger for other pathological changes, including:
- Infectious diseases. People with lupus are more vulnerable to infection because both the disease and its treatment can weaken the immune system.
- Oncological pathologies. With SLE, the risk of developing malignant tumors is slightly increased.
- Carrying out the bones. Lupus leads to disruption of the normal blood supply to the bones, which causes microfractures and destruction of bone tissue in general.
Is lupus dangerous during pregnancy?

SLE is not a reason to have an abortion.
Photo: user18526052 / freepik.com Despite the fact that lupus does not affect the ability to get pregnant, conceiving a child is recommended 6 months after the start of remission or after 3 months of complete control of the disease. Pregnant women with SLE are at increased risk of developing a number of complications. Among them:
- Exacerbations of lupus, which most often occur in the first and second trimester of pregnancy and are mild in nature.
- Preeclampsia and eclampsia are severe pathological conditions during pregnancy, characterized by preconvulsive or convulsive states caused by systemic hemodynamic disorders. Preeclampsia occurs in approximately 1 in 5 pregnant women with SLE.
- Premature birth, early and late miscarriages.
- The development of concomitant diseases, including diabetes, heart and kidney diseases.
However, most children born to mothers with lupus are healthy. Only in rare cases do infants develop a special form of the disease, neonatal lupus. In this case, the child may develop a skin rash, problems with the liver or hematopoietic system. As a rule, during the first 3-6 months of life, all symptoms disappear without a trace.