Despite its relatively small size, the cervix is a rather complexly organized organ, and its pathology is very diverse. The inside of the cervical (cervical) canal is lined with cells of single-layer columnar epithelium. It has many depressions - glands that produce mucus, the properties of which vary depending on the age of the woman and the phase of the menstrual cycle. Outside (from the vagina), the cervix is covered with a completely different layer of cells—stratified squamous non-keratinizing epithelium. It moves to the vaginal vault and lines the vaginal cavity from the inside. It has no glands and changes less during the menstrual cycle. The border between these two types of epithelium is most often located in the area of the external uterine pharynx (entrance to the cervical canal of the uterus) and is called the transformation zone (Fig. 1).
Figure 1. Zonal anatomy of the cervix.
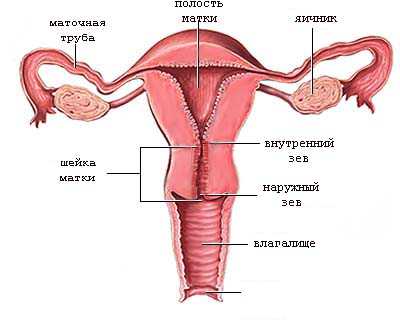
More than 90% of cervical neoplasia (precancerous condition) and cancerous lesions occur in the transformation zone.
What is “cervical erosion”?
The term "erosion" refers to a tissue defect. For example, we commonly call such a defect on the skin “abrasion.” True erosion of the cervix is extremely rare and is of a traumatic or radiation nature. For some reason, in Russian-speaking usage, in the old fashioned way, this term refers to any change in the cervix that is visible to the eye and has a brighter color than the usual mucous membrane. This is an outdated, incorrect term. It was used by gynecologists in the pre-colposcopic and pre-histological era, when any change in the cervix was regarded on the basis of examination as erosion and it was IMPOSSIBLE to make a more accurate diagnosis.
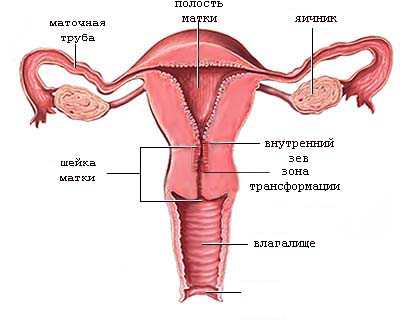
What lies behind the brightly colored “spot” in the area of the external uterine pharynx, which is found in every fourth woman of reproductive age, and which is called “congenital erosion”? As already mentioned, the border of two types of cellular lining of the cervix (single-layer cylindrical and stratified squamous epithelium) is most often located in the area of the external uterine pharynx (entrance to the cervical canal) and is called the transformation zone (Fig. 1). But this border is not fixed throughout a woman’s life. In all girls, before the onset of puberty, the border runs outward from the external pharynx, and then gradually shifts inward. In postmenopausal (menopausal) women, the transformation zone is located approximately at the border of the middle and lower third of the cervical canal (Fig. 2).
Figure 2. Cervical transformation zone.
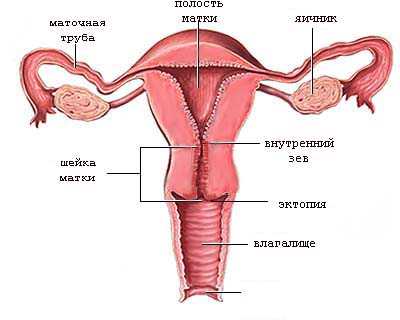
During reproductive age, due to individual variations, about a quarter of young women have an outward displacement of the transformation zone. Since single-layer cylindrical epithelium has a brighter color and a more “juicy” appearance, during a gynecological examination in the speculum it has a characteristic appearance, which doctors used to mistake for erosion. The correct name for this phenomenon is ectopia (or ectropion ), which literally translates as “located outside” (Fig. 3).
Figure 3. Localization of cervical ectopia.
The appearance of cervical ectopia is shown in Fig. 4.
Figure 4. Cervical ectopia.
Treatment
The treatment regimen can be determined after receiving the results of basic examinations:
- gynecological examination in speculum and bimanual examination;
- determination of the concentration of female sex hormones in the blood;
- general blood analysis;
- ultrasound examination.
Basic rules of therapeutic intervention:
- If the disease has an infectious basis, the treatment regimen necessarily includes antibiotics. The required medication and its dose are determined by the attending physician after an accurate determination of the pathogen. To increase efficiency, you need to take immunostimulants.
- For the development of non-infectious diseases, vaginal suppositories and capsules are used.
- If the cause is erosive damage to the cervix, the woman needs surgery. Treatment is provided by laser therapy, cryodestruction and radio wave treatment.
- Polyps and papillomas are removed surgically. After surgery, the use of antibacterial agents is indicated.
If the bleeding is contact and appears after sexual intercourse, ultrasound or gynecological examination, there is no need to worry. There is probably some minor damage to the mucous membranes. If blood from the vagina begins to flow heavily, its volume is commensurate with menstrual blood loss, you need to visit a gynecologist. It is not always possible to stop bleeding on your own.
Attention! The drug Dicynon or Vikasol will help stop the bleeding. The compositions are produced by pharmaceutical companies in the form of injection solutions and tablets. The patient must understand that such drugs are not suitable for constant use and help reduce the intensity of bleeding without affecting its cause.
A disease that causes blood loss must be treated comprehensively. The course of therapy may include traditional methods, when properly combined with drug therapy. Douching or other procedures can only be done as prescribed by a doctor.
Is “congenital” ectopia a pathology?
No. This is an individual feature. With age, most likely, the transformation zone will shift to the cervical canal. But even if this does not happen, nothing needs to be done. Previously, “cauterization of erosion” was performed for most women whose ectopia persisted after childbirth. Now this tactic is considered incorrect, since women are exposed to an unreasonable risk of even a small surgical intervention, which has more complications and side effects than even a very long-term existence of ectopia can bring. Therefore, today, treatment of ectopia without concomitant pathology is carried out only in the case of an extremely large area, especially with the transition to the vaginal vaults (this condition is called adenosis), and sometimes with increased secretion of glands, the ducts of which open on the surface of the ectopia. In a word, ectopia is not a disease or even a risk factor for the disease, and therefore is only subject to observation once a year for cytological control.
Urethral candidiasis in women
Urethral candidiasis in women most often occurs against the background of fungal infection of the vulva and vagina. From here, pathogenic microorganisms penetrate the wide and short urethra, where they settle and begin to grow new colonies. Urethral candidiasis can be acute or chronic. In the first case, inflammation is accompanied by severe, acute symptoms. Acute candidiasis responds well to drug treatment, but if therapy is absent or incorrect, the disease becomes chronic, characterized by periods of remissions and exacerbations.
If candidal urethritis is not treated, the risk of developing the following dangerous complications increases:
- cystitis;
- pyelonephritis;
- fungal bezoars in the urinary tract, disrupting the normal flow of urine;
- necrosis of renal tissue;
- intrarenal or perinephric abscess;
- acute renal failure.
What are Nabothian cysts (Ovula Nabothii)?
In the transformation zone, the flat epithelium gradually “creeps” onto the columnar epithelium, “closing” the ectopia. However, the excretory ducts of the glands may become closed, and the mucus they produce accumulates in the form of small cysts. These cysts can be multiple and range in size from 1 mm to 2 cm. Small cysts do not require any treatment. Only large (severely deforming the cervix) and continuing to grow cysts may require opening and evacuation of the contents. But this happens extremely rarely.
Diseases of the cervix include the following:
- Inflammation of the cervical canal (endocervicitis).
- Cicatricial post-traumatic (postpartum or postoperative) deformity.
- Human papillomavirus infection (HPV), including cervical condylomas.
- Cervical intraepithelial neoplasia (CIN) (Other names: dysplasia, dyskeratosis, squamous intraepithelial formation (SIL)) and cervical intraepithelial glandular neoplasia (CIGN).
- Cervical cancer: squamous cell carcinoma or adenocarcinoma.
- Endometriosis of the cervix.
- Polyps and fibroids of the cervical canal.
Read about diagnostic methods (colposcopy, targeted biopsy, cytological and histological studies) and treatment of precancerous diseases of the cervix (laser coagulation, cryodestruction, diathermoexcision, conization of the cervix) in the sections diagnostics, treatment and services.
- Inflammation of the cervical canal - endocervicitis . Most often it is caused by sexually transmitted infections (chlamydia, mycoplasma, gonococci) or nonspecific infections (streptococcus, staphylococcus, E. coli, corynebacteria, enterococcus, etc.). In the first case, infection occurs through sexual contact. The second group of microorganisms enters the cervix most often by lymphogenous (through lymphatic vessels) or contact (from the rectum) route; however, sexual intercourse is not necessary for their development, but can contribute to inflammation. Other provoking factors may be some benign diseases of the cervix (see below), cicatricial deformation of the cervix, weakening of general and local immunity. Endocervicitis is manifested by profuse mucous leucorrhoea, sometimes with an unpleasant odor. Endocervicitis can be one of the causes of miscarriage and premature birth. The disease can be suspected already during a gynecological examination: a large amount of mucus is released from the cervical canal, the transformation zone has a bright pink color. To diagnose the infection that caused the process, the following tests are taken: a smear for the degree of purity, culture for flora and sensitivity to antibiotics, testing for the presence of chlamydia, mycoplasma and ureaplasma (by PCR or culture), sometimes culture on special media to isolate trichomonas, fungus genus candida, gonococcus. Treatment for endocervicitis depends on what infection is causing it.
- Deformation of the cervix occurs due to traumatic childbirth or surgical interventions on the cervix. During labor, the cervix shortens, flattens, and then dilates to a diameter of 10 cm, allowing the fetal head to pass through the mother's birth canal. Sometimes, during the passage of the head, the cervix ruptures. This is facilitated by the following factors: rapid and rapid labor, weakness of labor with early ineffective pushing, inappropriate behavior of the woman in labor during pushing, which is often observed against the background of fatigue and painful contractions, the application of “high” obstetric forceps, a large fetus (weighing more than 4000 grams). ), previous operations on the cervix, including cervical excision, diathermocoagulation of ectopia, etc., ruptures in previous births. Most often, ruptures occur on the sides of the neck (at 3 and 9 o'clock). They can be of several degrees in depth. At the most severe degree, the ruptures reach the vaginal fornix and spread to the body of the uterus. After childbirth, the obstetrician examines the cervix “in the speculum” and, if ruptures are detected, closes them with absorbable sutures. Unfortunately, not all ruptures are diagnosed and carefully sutured. In such cases, the cervix after childbirth is formed defective - the cervical canal often remains gaping, and the cervix itself can take on the most bizarre shapes. If a woman is not planning a pregnancy, then nothing may bother her, and she will only find out about the presence of scars and deformities during the next gynecological examination. However, problems may arise during the next pregnancy - most often, spontaneous abortions (miscarriages) and premature births. There are extremely many reasons for spontaneous abortions, and cervical pathology is not the most common of them. However, cervical insufficiency can be suspected if the miscarriage occurs more than 16 weeks, begins with rupture of amniotic fluid, and there is a history of traumatic birth or cervical surgery. Diagnosis includes a visual examination in a gynecological chair, and, if necessary, cervicohysterography (X-ray examination with the introduction of a contrast agent into the lumen of the cervical canal and the uterine cavity). Treatment is required if a woman suffers from miscarriage due to severe deformation of the cervix. In such cases, surgical treatment is performed - cervical plastic surgery (tracheloplasty). If a cervical deformity is detected during pregnancy in the presence of signs of a threatening miscarriage, a special circular suture is placed on the cervix in order to preserve the pregnancy, designed to compensate for the lost mechanical function of the cervix. This suture usually remains until full term pregnancy. It is removed either on the eve of the expected birth, or in the event of the onset of labor.
- Papillomavirus infection (HPV) , including exophytic condylomas of the cervix.
 In short, you should know that: 1) the development of exophytic condylomas on the surface of the cervix, most often caused by papillomavirus type 6, leads to changes in the mucosa, which can be characterized as a mild degree of dysplasia (see point 4). 2) They themselves do not lead to the development of cancer and precancerous conditions of the cervix. 3) Small condylomas often undergo spontaneous regression (disappear on their own). 4) Oncogenic serotypes of HPV viruses (16, 18, 35, 39, 45) significantly increase the risk of developing severe dysplasia and cervical cancer. Moreover, they are the main cause of the development of these diseases. 5) Oncogenic types of viruses do not cause the development of exophytic condylomas. They are integrated into the genome of epithelial cells and change their genetic properties, promoting gradual cancerous degeneration. 6) Exophytic condylomas of large sizes, as a rule, must be removed (for example, using electrocoagulation, laser, podophyllotoxin preparations, etc.). 7) To date, there are no systemic medications that can reliably cure the papilloma virus. Detection of long-term persistence (preservation in the body) of oncogenic type papilloma viruses is the main risk factor for the development of severe degrees of dysplasia and cervical cancer, therefore, in this case, a particularly thorough and frequent examination of the cervix is required in order to detect the disease in time and adequately treat it.
In short, you should know that: 1) the development of exophytic condylomas on the surface of the cervix, most often caused by papillomavirus type 6, leads to changes in the mucosa, which can be characterized as a mild degree of dysplasia (see point 4). 2) They themselves do not lead to the development of cancer and precancerous conditions of the cervix. 3) Small condylomas often undergo spontaneous regression (disappear on their own). 4) Oncogenic serotypes of HPV viruses (16, 18, 35, 39, 45) significantly increase the risk of developing severe dysplasia and cervical cancer. Moreover, they are the main cause of the development of these diseases. 5) Oncogenic types of viruses do not cause the development of exophytic condylomas. They are integrated into the genome of epithelial cells and change their genetic properties, promoting gradual cancerous degeneration. 6) Exophytic condylomas of large sizes, as a rule, must be removed (for example, using electrocoagulation, laser, podophyllotoxin preparations, etc.). 7) To date, there are no systemic medications that can reliably cure the papilloma virus. Detection of long-term persistence (preservation in the body) of oncogenic type papilloma viruses is the main risk factor for the development of severe degrees of dysplasia and cervical cancer, therefore, in this case, a particularly thorough and frequent examination of the cervix is required in order to detect the disease in time and adequately treat it. - Cervical intraepithelial neoplasia (dysplasia) . This term (CIN) is used to refer to disorders of the maturation and structure of stratified squamous epithelium. Changes are assessed by cytological examination of cell scrapings from the surface of the neck and/or by histological examination of biopsy material. This pathology is associated with impaired cellular differentiation and maturation. There are three degrees of dysplasia: CIN I, CIN II, CIN III. With mild dysplasia (CIN I), cell maturation is impaired in the lower third of the epithelial layer. The top two thirds look typical. With the second and third degrees of dysplasia (CIN II, CIN III), cell maturation is impaired, respectively, in 2/3 or throughout the entire thickness of the epithelium. The next most severe cellular and tissue changes are carcinoma in situ, which translates as cancer “in place,” that is, within the epithelial layer, without growing into the underlying tissue of the cervix.
 In short, you should know that: 1) the development of exophytic condylomas on the surface of the cervix, most often caused by papillomavirus type 6, leads to changes in the mucosa, which can be characterized as a mild degree of dysplasia (see point 4). 2) They themselves do not lead to the development of cancer and precancerous conditions of the cervix. 3) Small condylomas often undergo spontaneous regression (disappear on their own). 4) Oncogenic serotypes of HPV viruses (16, 18, 35, 39, 45) significantly increase the risk of developing severe dysplasia and cervical cancer. Moreover, they are the main cause of the development of these diseases. 5) Oncogenic types of viruses do not cause the development of exophytic condylomas. They are integrated into the genome of epithelial cells and change their genetic properties, promoting gradual cancerous degeneration. 6) Exophytic condylomas of large sizes, as a rule, must be removed (for example, using electrocoagulation, laser, podophyllotoxin preparations, etc.). 7) To date, there are no systemic medications that can reliably cure the papilloma virus. Detection of long-term persistence (preservation in the body) of oncogenic type papilloma viruses is the main risk factor for the development of severe degrees of dysplasia and cervical cancer, therefore, in this case, a particularly thorough and frequent examination of the cervix is required in order to detect the disease in time and adequately treat it.
In short, you should know that: 1) the development of exophytic condylomas on the surface of the cervix, most often caused by papillomavirus type 6, leads to changes in the mucosa, which can be characterized as a mild degree of dysplasia (see point 4). 2) They themselves do not lead to the development of cancer and precancerous conditions of the cervix. 3) Small condylomas often undergo spontaneous regression (disappear on their own). 4) Oncogenic serotypes of HPV viruses (16, 18, 35, 39, 45) significantly increase the risk of developing severe dysplasia and cervical cancer. Moreover, they are the main cause of the development of these diseases. 5) Oncogenic types of viruses do not cause the development of exophytic condylomas. They are integrated into the genome of epithelial cells and change their genetic properties, promoting gradual cancerous degeneration. 6) Exophytic condylomas of large sizes, as a rule, must be removed (for example, using electrocoagulation, laser, podophyllotoxin preparations, etc.). 7) To date, there are no systemic medications that can reliably cure the papilloma virus. Detection of long-term persistence (preservation in the body) of oncogenic type papilloma viruses is the main risk factor for the development of severe degrees of dysplasia and cervical cancer, therefore, in this case, a particularly thorough and frequent examination of the cervix is required in order to detect the disease in time and adequately treat it. In turn, CIGN is an analogue of CIN, but refers to columnar epithelium. CIGN is judged by cellular atypia of the epithelial layer. Accordingly, adenocarcinoma in situ is distinguished as the most severe dysplasia. Cells of altered tissue (both squamous and cylindrical epithelium) look atypical, which is confirmed by cytological examination of scrapings from the surface of the cervix (Papanicolau smear). In them, the nucleus is enlarged, it has a lighter color, and the content of cytoplasm in the cell is reduced. In addition to the changes described, blood vessels also acquire a special structure: they come close to the surface, arranged in the form of loops, spirals and other elaborate shapes. This helps distinguish healthy tissue from pathological tissue during colposcopic examination of the cervix.
Discharge in pregnant women
Bloody discharge of varying degrees of intensity may also appear in pregnant women after a routine examination. Why is this happening? Often the cause is a careless inspection. The mucous membrane becomes loose during pregnancy and the slightest mechanical impact can injure it. The volume of discharge is small. The discharge stops on its own within 2-3 days.
Examination of the vagina may provoke bleeding in low placenta previa. This is a pathology in which the placenta is located in the lower parts of the uterus. Presentation can be complete or partial. Women with such a physiological feature require special attention. Vaginal examinations are performed only as a last resort, as this can cause excessive hemorrhage and placental abruption. A careless examination may result in a risk of miscarriage. Bleeding in this case may be accompanied by lethargy, nausea, and dizziness.
Important! In the third trimester, one of the reasons for the appearance of red or dark discharge may be the passage of a mucus plug. This is a harbinger of early labor. If the expected date of birth is far away, you should immediately contact a specialist.
Light spotting should not cause much concern if the blood is bright scarlet, the discharge is insignificant and there are no symptoms associated with the disease (itching, burning, swelling, redness, pain, high temperature). But if the next day after the visit to the gynecologist the bleeding has not stopped and discomfort appears, then you should see a doctor to determine the cause.
What can happen to dysplasia if it is not treated?
57% of CIN I spontaneously regress (“go away on their own”), 32% persist as CIN I for a long time, 11% progress to CIN II, CIN III, and only 0.5% progress to invasive carcinoma. Unlike mild dysplasia, CIN III turns into invasive cancer in 12% of cases within 2 years, and regresses quite rarely.
Is it possible to suspect the presence of CIN before visiting a gynecologist?
As a rule, no. CIN and CIGN have virtually no clinical manifestations. Therefore, you need to visit your doctor regularly (at least once a year) , even if there is absolutely nothing bothering you. The appearance of bloody discharge during sexual intercourse deserves special attention. If the cervix bleeds, this can be a very serious symptom, indicating a pronounced pathological process, including cancer. Other causes of bleeding after sexual intercourse may be inflammation, atrophy of the vaginal mucosa (for example, in postmenopausal women), and pathology of the uterine body. In women taking microdose hormonal contraceptives, this can be observed, among other things, due to thinning of the endometrium against the background of weak hormonal stimulation. All these reasons are temporary, harmless and easily removable. But, to exclude the most serious of them - cervical diseases, all women with spotting after sexual intercourse are advised to immediately visit a gynecologist.
Cervical cancer . This is a dangerous malignant disease. Every year, about 400,000 are detected worldwide. new cases of cervical cancer, of which about 200,000 are fatal. Cervical cancer ranks third among cancer pathologies in women, second only to breast and uterine cancer. Squamous cell carcinoma develops from squamous epithelium, and adenocarcinoma, which has a high degree of malignancy (tendency to rapid growth and metastasis), develops from cylindrical epithelium.
The average age for the onset of squamous cell carcinoma is 46 years, for adenocarcinoma - 35 years. Often, malignant pathology of the cervix in women at risk develops even earlier - at the age of 24 years. According to the degree of invasion (germination of layers located under the epithelium), cancer is divided into carcinoma in situ, minimally invasive, and invasive cancer. Invasive cancer has 4 stages, depending on invasion into neighboring organs, involvement of regional lymph nodes and the presence of distant metastases (bones, liver, brain). The 5-year survival rate for the first stage is 85%, with 4 - 5%. Given the questionable prognosis and complex combination treatment of invasive cancer, the primary focus of public health in developed countries is on the early diagnosis of precancerous lesions and carcinoma in situ. In particular, in the USA, since 1960, it has now been possible to reduce mortality from cervical cancer by 87%, thanks to an established screening system (see the services section). If you want to protect yourself from developing incurable stages of cervical cancer, visit your gynecologist annually and undergo a special examination!
Who is at risk for developing dysplasia and cervical cancer?
- Carriers of HPV oncogenic serotypes (16, 18, 31, 45, and about a dozen intermediate-risk viruses)
- Long-term persistence of oncogenic types of virus (more than 2 years)
- High “viral load”, i.e. a large number of serotypes and their high concentration in tissues at the same time.
- Early onset of sexual activity
- Many sexual partners throughout life
- Smoking
Endometriosis of the cervix . Genital endometriosis is an extremely common disease in women of reproductive age. The most common locations of the lesion are the body of the uterus, ovaries, pelvic peritoneum, and uterosacral ligaments. The cervix accounts for only an extremely small percentage of endometrioid heterotopias. The cause of endometriotic lesions of the cervix is diathermocoagulation of ectopia, damage during surgical abortion, childbirth. On the relatively deep wound surface, pieces of endometrial tissue, released during the next menstruation, attach and “take root.” Cervical endometriosis usually manifests itself in the form of bleeding on the eve of menstruation. Diagnosis is carried out on the basis of a visual gynecological examination and colposcopy. Treatment is surgical and is necessary only for large heterotopias and in the presence of clinical manifestations. To remove heterotopias, their laser vaporization is used.
Polyps and fibroids of the cervical canal . The reasons for the appearance of polyps are not completely clear. Their structure is characterized by a central connecting stalk, covered with either stratified squamous or columnar epithelium. Most often, polyps are an accidental finding during a regular gynecological examination. If they are large, they can bleed easily. Polyps are a benign disease. However, sometimes cancer (especially adenocarcinoma) can have the appearance of a polyp. Such a polyp, as a rule, has an unevenly colored bumpy surface and bleeds easily. The presence of a polyp is an indication for its removal, followed by diagnostic curettage of the cervical canal and uterine cavity. Histological examination of the obtained material is important. Often, at the same time as a polyp of the cervical canal, a polyp or endometrial hyperplasia is detected.
Fibroids (myomatous nodes) of the cervix are less common than in the body of the uterus (see section “uterine fibroids”). They can also be subserous, intramural and submucosal. The presence of cervical fibroids in the vast majority of cases is an indication for surgical treatment. In the case of submucosal nodes, they are removed (with a scalpel or an electrocoagulator). Large intramural and subserous nodes quickly disrupt the anatomy and function of adjacent organs (bladder, ureters, rectum), and therefore are also an indication for one or another operation (conservative myomectomy, hysterectomy). The latter can be performed using either abdominal or vaginal access.
Bleeding due to uterine fibroids, adenomyosis, endometrial and cervical canal polyps
Uterine fibroids, endometriosis and polyps and endometrial hyperplasia are diseases associated with benign growth of uterine tissue. They appear most often during reproductive age.
All this pathology is easily diagnosed using ultrasound. As a rule, no additional examination methods are required. You can read about possible treatment options for uterine fibroids in the corresponding section of the website www. ya-zdorova.ru. In the presence of pathology of the uterine cavity, hysteroscopy with the appropriate amount of surgical intervention is indicated to eliminate the cause of bleeding.
Where to go for diagnosis and treatment of cervical diseases?
The medical institution to which you should contact must have an adequate diagnostic base. All types of cytological and histological studies should be available here. A highly qualified pathologist (histologist) must be well versed in all types of epithelial lesions, from the most minor and benign, to precancerous (such as CIN) and malignant. The institution must have PCR diagnostics available (including for detecting papillomavirus infection and its typing), there must be all the necessary instruments for high-quality collection of materials for research (special disposable brushes, spatulas), there must be special standard instruments for cervical biopsy uterus, there must be electrosurgical equipment for conization of the cervix. The gynecologist must have a high-quality colposcope and be fully proficient in the techniques and methods of colposcopy. Doctors at a clinic specializing in the treatment of cervical diseases must have access to and master methods of excision and destruction of affected tissue (electrocoagulation and excision, laser coagulation or evaporation, cryodestruction). If necessary, doctors must also perform surgical excision (“cold knife”) of the affected tissue with the application of cosmetic sutures. Ideally, the medical institution you choose should have sufficient administrative and computer facilities to track and monitor patients at high risk for developing cervical cancer. Remember that the widespread introduction in developed Western countries of preventive cytological examinations of cervical smears stained with Papanicolaou, as well as other components of the treatment and preventive program for cervical diseases, has reduced the incidence of cervical cancer by 87%. THIS IS THE BASIS OF THE SIGNIFICANT INCREASE (BY 15 YEARS) IN THE AVERAGE LIFE EXPECTATION OF WOMEN IN WESTERN EUROPEAN COUNTRIES, JAPAN AND THE USA IN RECENT YEARS.
Causes of development of uterine candidiasis
A decrease in the body’s protective functions and an imbalance of microflora are provoked by the following negative internal and external factors:
- candidiasis in the vagina or intestines;
- often recurrent chronic infectious processes;
- hormonal and endocrine disorders;
- promiscuous sex, unprotected sex life;
- frequent abortions;
- uncontrolled use of antibacterial, hormonal agents, immunosuppressants, cytostatics;
- curettage for diagnostic purposes, injuring the cervix;
- surgical treatment of abdominal organs;
- frequent douching;
- wearing synthetic underwear;
- tight clothes;
- failure to comply with intimate hygiene rules.











