Get tested at a discount in the online store
Kurzrock-Miller cross test Postcoital test MAR test
The immune system plays an important role in human reproduction. Immune cells and their secretion products are involved in the process of ovulation, preparation of the endometrium for implantation of a fertilized egg, gamete interaction and the development of normal pregnancy. Changes in immune homeostasis can disrupt the normal reproductive process and lead to decreased fertility, miscarriage and infertility. It was found that 20% of couples with unexplained infertility have immune factors.
One of the immunological factors leading to infertility is the formation of antisperm antibodies. Ramck and Wilson first reported the presence of antisperm antibodies in infertile men in 1954. Since that time, interest in studying the role of antisperm antibodies in disrupting reproductive processes has not waned. In recent years, thanks to the improvement and spread of assisted reproductive technologies, it has become possible to study the participation of antisperm antibodies in the process of conception, at the level of interaction between the sperm and the egg. Antisperm antibodies are found in 9-36% of infertile couples, compared with 0.9-4% of couples having children.
Antisperm antibodies are immunoglobulins of the IgG, IgA and/or IgM isotypes, which are directed against sperm membrane antigens. Antisperm antibodies are polyclonal (diverse), which is determined by the presence of different target antigens (various antigens have now been identified, such as YWK II, BE-20, rSMP-B, BS-63,BS-17, HED-2 and 75-kDa ) and thus immunological infertility is a consequence of the combined effects of various antisperm antibodies. Antisperm antibodies are formed in various parts of the reproductive tract of both men (testes, epididymis, vas deferens) and women, they are directed against different parts of the sperm (sperm head, tail, middle part or a combination thereof), can be present in varying quantities and have an impact on reproductive processes in various ways. The detection of antisperm antibodies in the cervix indicates their presence in other parts of the reproductive tract (in the uterine cavity and in the lumen of the fallopian tube). It became clear that antisperm antibodies in a woman affect not only the passage of sperm through the cervix, but also sharply worsen the quality of fertilization.
Formation of antisperm antibodies in men
Because sperm is not produced in the body until puberty, specific sperm antigens are not recognized as “self” by the immune system. However, sperm are not attacked by the immune system, since they are protected from contact with cells of the immune system circulating in the bloodstream by several physiological mechanisms.
The first mechanism is the existence of a biological barrier between the seminiferous tubules and blood vessels, the so-called blood-testis barrier. It is formed by tight junctions between Sertoli cells and the basement membrane. The blood-testis barrier protects testicular cells from immune cells entering the spermatic cord.
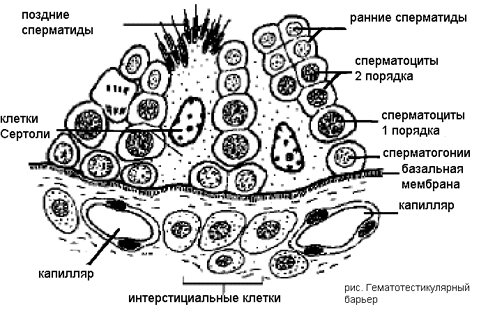
However, a small number of sperm and their precursors can cross the blood-testis barrier and enter the blood, thereby triggering an immune response against sperm, so there are immunological defense mechanisms:
- Immunological tolerance due to a low threshold for the penetration of sperm antigens.
- Immunomodulatory mechanisms within the testes, such as steroids, macrophages, suppressor cells, which can prevent activation of immunological recognition.
- Peripheral immunomodulation of the testes: T-suppressor cells in the epididymis (epididymis) and immunosuppressive activity of seminal fluid (in sperm there is a component called “immunoglobulin binding factor” Immunoglobulin binding factor - IBF which is supposed to reduce the activation of B-lymphocytes or suppress T-lymphocyte activity helper cells, thus preventing the production of antisperm antibodies in the reproductive tract).
Disturbances of the blood-testis barrier, such as injury, infection, or surgery, can trigger the entry of circulating immune cells into the male genital tract and expose sperm to the immune system. When this occurs, the suppressive activity of T cells may be suppressed primarily by the production of antibodies to sperm. Men who have had a vasectomy are an example of this problem. Many of them have antisperm antibodies (more than 65%).
Risk factors for the development of antisperm antibodies in men are:
- Injury;
- Varicocele (dilation of the veins surrounding the spermatic cord);
- Blockage of the vas deferens;
- Infections;
- Oncology;
- Cryptorchidism;
- Surgical operations;
Formation of antisperm antibodies in women
Education mechanisms:
- Violation of the integrity of the mucous membranes (chemical methods of contraception).
- High numbers of leukocytes, including lymphocytes, in sperm.
- Sperm associated with antisperm antibodies.
- High percentage of abnormal and “old” sperm (with rare sexual activity).
- Oral and anal sex (sperm enters the gastrointestinal tract).
- Entry of a large number of sperm into the abdominal cavity (features of the morphology of the genital tract, incorrect implementation of intrauterine insemination methods).
- IVF attempts in the past (hormonal “shock” to the hypothalamic-pituitary-ovarian axis, trauma during egg retrieval).
- Coagulation of cervical erosion in the past.
Despite the presence of “foreign” sperm cells during sexual intercourse, the production of antisperm antibodies in women usually does not occur. Like the cells of the male genital tract, the cells lining the vagina serve as an effective physiological barrier and limit the presentation of sperm components to the immune system. In addition, seminal fluid contains high levels of prostaglandin E2, a potential immune suppressor, as well as "immunoglobulin binding factor" - IBF, which prevents the production of antisperm antibodies in the reproductive tract. Similarly as in men, infection or inflammation can increase the chance that a woman will develop immune recognition of sperm.
Why do antisperm antibodies appear in the female body?
Sperm and seminal fluid entering a woman’s reproductive system during sexual intercourse are completely foreign. However, normally they do not encounter any insurmountable obstacles on the way to the egg, easily and naturally fertilizing it during the process of fusion. However, such an idyllic picture is not always real - in some cases, a woman’s immunity exhibits pathological activity, synthesizing anti-sperm antibodies and attacking sperm during movement, completely destroying or significantly weakening them. This pathology can occur as a result of the following deviations:
- inflammation of the reproductive organs that occurs against the background of infection and activates the immune defense, which subsequently acquires hypertrophied forms;
- entry into a woman’s body of defective, non-viable and abnormal sperm, which automatically trigger protective mechanisms, preventing an obviously unpromising pregnancy;
- a high percentage of leukocytes in the partner’s seminal fluid, which occurs against the background of infection and is perceived by the female body as potentially dangerous;
- frequent use of chemical methods of contraception, which can cause damage to the vaginal mucosa;
- structural features of the female genital organs or the consequences of unsuccessful intrauterine insemination, as a result of which a high dose of sperm penetrates the abdominal cavity;
- atypical reaction to coagulation of erosive lesions of the vaginal mucous membranes;
- unsuccessful attempts at in vitro fertilization, which caused a hormonal storm and atypical immune reactions.

Any of these diseases can be complicated by the appearance of antisperm antibodies, which aggravate reproductive difficulties, causing immunological infertility. However, this list is far from complete - there can be an infinite number of factors that in one way or another influence the reactions of women’s immunity, and taking each of them into account is an almost impossible task. That is why the diagnosis of each reproductive problem begins with a blood test of the patient, which serves as a reliable diagnostic criterion for the presence of ASAT in a woman.
The influence of antisperm antibodies on reproduction processes
For a long time, it was unclear how antisperm antibodies could affect reproductive processes. Currently, numerous studies have shown that the effect of antisperm antibodies is quite diverse; the following mechanisms are known:
- decreased sperm motility, disruption of their functional activity,
- blockade of sperm penetration into cervical mucus,
- influence on such important stages of sperm preparation for fertilization as capacitation and acrosomal reaction (link.)
- impact on the process of fertilization of an egg by a sperm (interaction between a sperm and an egg),
- influence on the process of implantation of the blastocyst (fertilized egg),
- inhibition (suppression) of the growth and development of the embryo.
Classification and features of ACAT
Antisperm antibodies are substances of protein origin that are able to recognize sperm and have a destructive effect on them. By attaching to sperm membranes, ACAT can cause the following cellular abnormalities:
- Sperm immobilization is the partial or complete immobilization of male germ cells in the female reproductive tract.
- Sperm agglutination is the gluing of sperm to each other, macrophages, cervical mucus, cell particles and other elements contained in female vaginal discharge.
- Spermolysis is the total destruction of male gametes.
Any of the possible actions of antisperm antibodies can significantly complicate conception, leading to infertility. However, in some cases, this feature does not prevent pregnancy - according to statistics, in 1-4% of married couples with children, a low concentration of ACAT is found in the mother’s blood, which she did not even suspect before pregnancy. This means that this feature is not a death sentence for a woman - with proper treatment, the likelihood of defeating the immunological factor of infertility is very high.

Decreased sperm motility
Antisperm antibodies, fixing on the sperm membrane in various areas (sperm head, middle part, tail) have an inhibitory effect on sperm, both during their movement in the male reproductive tract and in the female.
Antisperm antibodies can cause agglutination (“gluing”) and immobilization (immobilization) of sperm. The extent to which sperm motility will be reduced will depend on the amount of antisperm antibodies (there must be a high titer of antibodies), as well as on the place of their fixation. The most unfavorable site for fixation of antisperm antibodies is the head of the sperm.
Blockage of sperm penetration into cervical mucus
The fact that in case of infertility one of the causative factors is the blockade of sperm penetration into the cervical mucus is well known. Studies have shown that the presence of antisperm antibodies interferes with or blocks the penetration of sperm into the cervical mucus. The phenomenon of “shaking in place” of sperm coated with antisperm antibodies has been described. It is assumed that it is caused by the interaction of the Fc regions of antibodies with glycoprotein micelles of cervical mucus. This sign can be observed during a postcoital test in vivo (Shuvarsky-Sims-Hüner test) and in vitro (Kurzrock-Miller test) (link).
Effect on fertilization
Antisperm antibodies interfere with the interaction of gametes (sex cells). They prevent sperm from penetrating the zona pellucida of the egg. Although the mechanisms of this have not been fully elucidated, it is reliably known that antisperm antibodies suppress the acrosomal reaction of sperm, which is a necessary condition for successful fertilization. If a husband or wife has antisperm antibodies, the quality of the resulting embryos deteriorates, which reduces the likelihood of success in infertility treatment using in vitro fertilization. If treatment of ASAT with conservative methods fails, the more preferable method of treating infertility in such couples is ICSI (introducing sperm into the egg).
What are antibodies
The formation of antibodies is a universal mechanism for protecting the body (immune system) from foreign agents - viruses, bacteria, tumor cells. Antibodies are formed to substances that are “recognized” by cells of the immune system as foreign. If for some reason the sperm membrane also becomes “foreign” for the body, antibodies of several classes are produced to them:
- Class A immunoglobulins (IgA) are produced by special cells of the mucous membranes and are responsible for local immunity.
- Immunoglobulins G (IgG) - are produced later, but remain for life, playing a major role in neutralizing antigens.
- Immunoglobulins M (IgM) are the first to be synthesized during the immune response, but last only 14 days. Therefore, they are not detected in the MAR test.
Antibodies to sperm (antisperm antibodies (ASAT)) of various classes circulate in the blood and are found in large quantities in semen or cervical mucus in women. They attach (“stick”) to sperm and prevent fertilization of the egg.
Influence on the processes of implantation, growth and development of the embryo
At one time it was assumed that ASAT could have a negative effect on the development of the embryo in the short term. Recently, most researchers do not agree with such views.
Indications for testing for antisperm antibodies are:
1. Changed spermogram parameters:
- aggregation and agglutination of sperm;
- low mobility;
- phenomenon of “moving in place” of sperm
- low sperm viability;
2. Deviations in the postcoital test:
- a small number of sperm in the cervical mucus;
- low mobility;
- the phenomenon of sperm trembling in the postcoital test;
- negative postcoital test;
3. Negative test for the interaction of sperm and cervical mucus in vitro.
4. The presence of certain risk factors (see above);
5. Failures or low rates of IVF;
6. Unexplained infertility in the examined couples.
3.What are the risks and what may affect the analysis?
What are the risks of antisperm testing?
If you take a blood test for antibodies, then possible risks may be associated only with blood sampling. In particular, the appearance of bruises at the site of blood sampling and inflammation of a vein or artery (phlebitis). Warm compresses several times a day will relieve phlebitis. If you are taking blood thinning medications, you may bleed at the puncture site.
If you are undergoing a sperm analysis, there are no risks associated with this procedure.
What can interfere with antisperm analysis?
If a man last ejaculated less than two days before the test or more than five, this may throw off the test results.
Methods and media for the determination of antisperm antibodies
In men, it is better to detect antisperm antibodies in semen. Determination of ASAT in blood plasma is an addition to semen analysis. In case of azoospermia (lack of sperm in semen), the most informative is the determination of ASAT in blood plasma. ACAT can belong to different classes of immunoglobulins (M, G, A), but the most important is the determination of IgG, which easily passes through biological barriers, and IgA (secretory immunoglobulins). In women, antisperm antibodies should be determined both in cervical mucus and in blood plasma. It is mandatory to determine antisperm antibodies in couples preparing for IVF, especially if women's plasma will be used as a cultural medium in IVF technologies. In men with high titers of antisperm antibodies, especially on the head of the sperm, assisted reproductive technologies such as ICSI (intracytoplasmic sperm injection ICSI) may be offered.
The most commonly used methods for determining antisperm antibodies are based on the determination of antibodies directed against various membrane antigens. There is no “gold standard” for determining antisperm antibodies. Therefore, the methods used to determine them are complementary.
At CIR Laboratories LLC, an extensive examination of the couple is carried out to exclude male and cervical factors of infertility. The specialists of our spermatology laboratory have been dealing with these issues for many years, and currently we can offer a very high-quality examination at the most modern level. Determination of antisperm antibodies at CIR Laboratories LLC
Methods for diagnosing immunological forms of infertility associated with the production of ASAT are:
1. Postcoital test, or test for the interaction of sperm with cervical mucus. It is carried out in two versions:
- In vivo
test (Shuvarsky-Sims-Hüner test). The patient comes for the study after sexual intercourse in the days preceding ovulation. The contents of the vagina and cervix are examined. Although the acceptable period between sexual intercourse and the study is 24 hours, we recommend performing this test 3-12 hours after sexual intercourse. A negative (“bad”) test occurs when sperm motility in a woman’s genital tract often decreases. - In vitro
test (Kurzrock-Miller test). Spouses come for the study in the days preceding ovulation. The husband donates sperm, and a drop of cervical mucus is taken from the wife. The interaction of sperm and cervical mucus is assessed under a microscope. A negative (“bad”) test result is a decrease in the forward movement of sperm in the cervical mucus.
It should be remembered that the most common reason for a negative post-coital test is the presence of ACAT in the semen (i.e. the problem is related to the husband), and not in the cervix. However, very often there is a combination of the role of both male and female factors. The postcoital test is one of the most capricious tests in infertility testing. The percentage of false results in this study is quite high. Therefore, the postcoital test must be supplemented with special studies on ASAT.
2. MAR test. A test that determines the percentage of sperm associated with antibodies of the IgG and IgA classes (direct MAR test) and the titer of antisperm antibodies in biological fluids (sperm plasma, cervical mucus, blood plasma) (indirect MAR test). The test is the internationally recognized standard for the diagnosis of ACAT. The test has high specificity, but not always high sensitivity.
3. Immunobead test. It is analogous to the MAR test. The spectra of antibodies detected by MAR and immunobead tests do not always match, which explains the often observed discrepancies between test results in the same patient.
4. The latex agglutination test is rarely performed.
5. Enzyme-linked immunosorbent method (ELISA). Method commonly used for the determination of AST in blood plasma. It is an additional method for diagnosing ASAT. High titers of ASAT determined by ELISA in the blood of women are not always associated with a worsening prognosis of pregnancy.
general description
Indication of antibodies to sperm antigens is an additional test in the diagnosis of immunological causes of male and female infertility.
Antisperm antibodies, in addition to blood serum, can also be found in cervical mucus, seminal plasma, and on the surface of sperm. Normally, there are no antisperm antibodies (AS) in the blood serum. Women normally do not produce antibodies against sperm antigens (Ags), however, various causative factors (bacterial and viral infections, autoimmune diseases) can lead to loss of immunological tolerance. The immune response in women most often manifests itself at the level of the cervix, and lastly in the vagina, endometrium and fallopian tubes. It is believed that recognition of sperm antibodies by the woman's immune system is critical for the normal process of fertilization and fetal development in the early stages of pregnancy. Normally, in the absence of antibodies in the blood, under the influence of sperm antibodies, the immunocompetent cells of a pregnant woman produce cytokines that promote the formation of trophoblast, the growth and formation of the placenta, and implantation. If antisperm antibodies are present in a woman’s blood, these processes are disrupted, which leads to miscarriage, gestosis, delayed fetal development, and fetoplacental insufficiency. At the same time, it is usually not possible to identify a clear correlation in women between the concentration of AT in the blood serum and the prognosis for fertility.
Antisperm antibodies to surface Ags of sperm are found in women not only in the blood serum, but also in the cervical mucus, where they can damage or agglutinate sperm, which prevents the fusion of the sperm with the egg and conception.
It does not seem important whether antisperm antibodies occur in the male or female body, since in any case they negatively affect sperm to the same extent. The presence of antisperm antibodies in the male body causes autoimmune infertility. In women in such a situation, immunological incompatibility of partners is diagnosed.
Antisperm antibodies are found in about a quarter of infertile families. The pathological effects of antisperm antibodies depend on their titer and direction against various antigens on the surface of sperm. The presence of antisperm antibodies in spouses is not necessarily accompanied by infertility, but among couples with their presence in at least one of the spouses, the pregnancy rate is recorded almost half as often. The presence of antisperm antibodies is considered the main cause of infertility if other causes are excluded during examination. It is known that approximately a fifth of unexplained infertility is associated with immunological reasons, the main one of which is the presence of antisperm antibodies in one of the partners.
Risk factors for the appearance of antisperm antibodies in women:

commitment to anal or oral sex;- unsuccessful attempts at in vitro fertilization in the past;
- entry of sperm into the abdominal cavity during the intrauterine insemination procedure;
- violation of the integrity of the mucous membrane of the internal genital organs;
- use of chemical contraception methods;
- increased number of leukocytes in the partner’s sperm;
- the presence of antisperm antibodies in the partner’s sperm;
- rare sexual intercourse;
- history of allergies;
- physiological decrease in immunity during ovulation;
- after coagulation of cervical erosion.
The results of the study for the presence of antisperm antibodies are taken into account when choosing infertility treatment tactics.
In men, antisperm antibodies are formed as a result of an autoimmune reaction to the spermatogenic epithelium. Causal factors contributing to the development of such a reaction include testicular trauma, bacterial and viral infections, testicular surgery (after vasectomy, antisperm antibodies are detected in all men), and in some cases it is not possible to determine the cause. To determine antisperm antibodies, the ELISA method is currently used, which is highly sensitive and specific, and also allows the determination of antibodies of different classes (IgA, IgM and IgG). The study of antisperm antibodies of various classes makes it possible to quantify the severity and severity of the autoimmune process; in addition, in men, the concentration of antisperm antibodies in the blood serum correlates with the prognosis for the restoration of fertilization ability. The presence of antisperm antibodies in sperm and blood serum negatively affects the genesis, motility, viability of sperm and, accordingly, the possibility of fertilizing a woman’s egg.
Risk factors for the appearance of antisperm antibodies in men:
- varicocele;
- vesiculitis;
- testicular injury;
- injuries and surgical interventions on the genitals;
- testicular surgery;
- infectious inflammatory diseases of the testicle;
- prostate infections;
- obstruction of the vas deferens;
- cryptorchidism;
- inguinal hernia;
- testicular cancer.
Determination of antisperm antibodies is carried out using the enzyme immunoassay method - ELISA. The samples are diluted and placed in a microplate, the wells of which are coated with a mixture of proteins that can interact with antibodies. Antisperm antibodies that are in the sample bind to these proteins, after which the optical density of the contents of the cells is measured, which is proportional to the concentration of antisperm antibodies. Determination of antisperm antibodies in blood plasma is very informative in both men and women. In particular, the study is prescribed if there are no sperm in the man’s semen. However, in males, preference should be given to the determination of antisperm antibodies in semen as the main test. Their determination in blood plasma should be an addition to semen analysis. It makes sense to carry out detection of antisperm antibodies in men as an additional study when changes in the spermogram or deviations in the postcoital test are detected.
Who should take a blood test for antisperm antibodies?
Blood samples for this test are taken from both men and women.
Preparing for analysis
No special preparation is required. It must be remembered that at least four hours must pass between the last meal and blood sampling.
How is the procedure performed?
Blood sampling is carried out as standard from the ulnar vein in the morning on an empty stomach.
Diseases and conditions for which a doctor may prescribe a test:
- unexplained infertility of a married couple with normal standard examination results;
- changes in spermogram;
- changes in postcoital test;
- negative cervical fluid-sperm interaction test;
- preparation for IVF;
- unsuccessful IVF attempts.
Decoding the analysis results
Exceeding normal test values is a probable factor of infertility. If, with an increased level of antisperm antibodies, pregnancy does occur, then the risk of their negative impact on the viability of the fetus is very significant.
With test threshold values of the order of 55–60 U/ml, it is advisable to repeat it after 2 weeks.
Treatment methods
Treatment of married couples with a detected increase in ACAT levels is carried out differently, depending on the entire complex of examination data. They usually start with the use of a barrier method (condom) continuously for a period of 3-6 months or intermittently (sexual activity without a condom only on days favorable for pregnancy). Reducing the flow of sperm into a woman’s body reduces the production of antibodies and increases the chances of pregnancy. In parallel, therapy can be prescribed that reduces the viscosity of cervical mucus (guaifenesin) and suppresses the production of ASAT in spouses. If conservative therapy fails, courses of intrauterine insemination with the husband's sperm or in vitro fertilization (IVF) are carried out. A contraindication for intrauterine insemination with the husband's sperm is the presence of ASAT in the husband, directed against the head of the sperm and not amenable to treatment with conservative methods. If these methods fail, you should move on to ICSI.