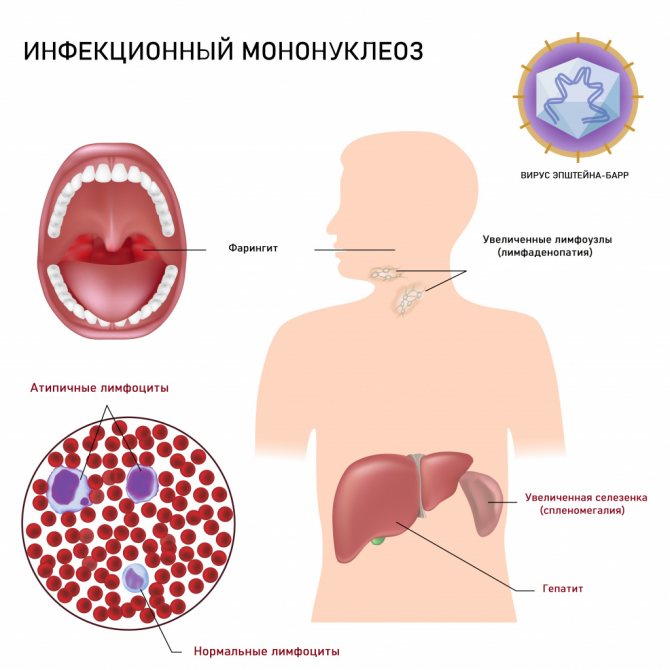
Epstein-Barr virus (EBV) has a complex structure and a variety of clinical forms of infection, so its diagnosis is difficult. Being a herpes virus, EBV is widespread, remains in the body for life and is most active in immunodeficiency states, which is why it is dangerous. In most cases, the primary infection is mild or asymptomatic. The classic manifestation (in only 20% of cases) is in the form of mononucleosis: high fever, enlarged cervical lymph nodes, sore throat, less often with an enlarged liver and spleen. During this period, the virus itself can be detected in blood, saliva and other biological fluids. Further, the viral infection can proceed as a long-term, often recurrent cold with a slight increase in temperature up to 37 degrees, weakness, and fatigue. In more severe cases, neurological manifestations, skin rashes, and respiratory complications occur. EBV carriage is associated with the development of lymphomas and tumors of the nasopharynx. Typically, antibodies to the Epstein-Barr virus are determined to clarify the stage of the disease and the duration of the process.
The presence of antibodies to the nuclear antigen IgG indicates that the Epstein-Barr virus has been in the body for a long time - more than 4 months. These antibodies are the last to be synthesized and remain in the body for life, so their detection with ambiguous symptoms suggests that the cause of the disease is EBV, which persists for a long time in the body or is undergoing a period of its reactivation. These antibodies are also considered as markers of past infection.
Meaning of test results.
No antibodies detected:
- Early period of infection. In case of clinical suspicion, determination of IgM to the capsid antigen or detection of EBV DNA by PCR is recommended.
- No EBV infection.
Antibodies detected:
- Confirms the presence of antibodies to the Epstein-Barr virus in the body, the infection is more than 4 months old.
Questionable result:
- Possibly if the level of antibodies is insufficient for a positive result. It is recommended to study IgM to the capsid antigen and repeat the study of IgG to the EBV nuclear antigen over time after 1 week.
Epstein–Barr virus
Hepatitis
Herpes
21150 November 12
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Epstein–Barr virus: causes, symptoms, diagnosis and treatment methods.
Definition
The Epstein-Barr virus (EBV) is present in most people, remaining in the body of a person who has been ill for life and being a trigger for various diseases. It is known that in many cases, primary contact with EBV occurs in the first decade of life, causing a persistent (persistent) infection. In early childhood, the disease is usually asymptomatic or with scant symptoms. Primary EBV infection at 10-20 years of age causes respiratory infections in 40% of cases, and infectious mononucleosis is diagnosed in 18-25% of patients.
Epstein-Barr virus can infect various types of cells, including immune system B cells (a type of white blood cell) and mucosal epithelial cells.
EBV is a member of DNA viruses from the Herpesviridae
(herpesviruses), subfamilies of gammaherpesviruses and genus lymphocryptoviruses. During the process of virus replication (self-copying), over 70 different virus-specific proteins are expressed. Currently, groups of immunogenic proteins have been identified, the determination of antibodies to which makes it possible to differentiate the stage of infection (EA - early antigen, EBNA-1 - nuclear antigen, VCA - capsid antigen, LMP - latent membrane protein).

Causes of diseases caused by the Epstein-Barr virus
The virus can spread from person to person through body fluids (airborne transmission). That's why infectious mononucleosis, one of the best-known diseases caused by EBV, is called the "kissing disease."
Another method of infection is through household contact (the virus is transmitted through toothbrushes, cutlery, towels, etc.). EBV can also be spread through blood and semen.
EBV multiplies in B lymphocytes and epithelial cells, and therefore there is a variety of clinical manifestations of this pathology. An important distinguishing feature of the virus is that it does not inhibit or disrupt the reproduction of B lymphocytes, but, on the contrary, stimulates it. This is the peculiarity of the pathogen - it multiplies in the cells of the immune system, forcing them to clone their own viral DNA.
The chronic inflammatory process caused by EBV leads to structural and metabolic disorders of the affected tissues, which is the cause of various somatic pathologies.
Classification of Epstein-Barr virus
There is no unified classification of Epstein-Barr virus infection (EBVI); the following is proposed for use in practical medicine:
- by time of infection - congenital and acquired;
- according to the form of the disease - typical (infectious mononucleosis) and atypical: erased, asymptomatic, with damage to internal organs;
- according to the severity of the course - mild, moderate and severe;
- according to the duration of the course - acute, protracted, chronic;
- by activity phase – active and inactive;
- mixed infection - most often observed in combination with cytomegalovirus.
Symptoms of the Epstein-Barr virus
Below is a partial list of diseases with which the Epstein-Barr virus is associated.
- Infectious mononucleosis (glandular fever, Filatov's disease) is a common infectious disease, the main manifestations of which are a rise in temperature to high values, enlarged lymph nodes, inflammation of the mucous membrane of the pharynx, enlargement of the liver and spleen. EBV in this case penetrates the epithelium of the mucous membranes of the upper respiratory tract.
- Lymphogranulomatosis (Hodgkin's disease) and some types of non-Hodgkin's lymphomas are a group of diseases united by malignant monoclonal proliferation of lymphoid cells in the lymph nodes, bone marrow, spleen, liver and gastrointestinal tract.
- Chronic fatigue syndrome is a condition characterized by a prolonged feeling of fatigue that does not go away after prolonged rest.
- Alice in Wonderland syndrome is a condition whose clinical manifestation is a violation of the sensation of one’s body and its individual parts. A person feels himself or parts of his body to be very large or very small compared to reality.
- Hepatitis caused by EBV is often a complication of infectious mononucleosis. Weakness, nausea, yellowness of the skin and mucous membranes appear, and the liver enlarges.
- Herpetic infection in the form of a genital or labial (on the lips) lesion. Stomatitis caused by EBV is also possible. When the infection is activated, a burning sensation and pain appear, followed by many small blisters.
- Post-transplant lymphoproliferative disease is a secondary malignant disease that develops after hematopoietic stem cell transplantation (a treatment method used for oncology, blood diseases, etc.), associated with EBV infection.
- Multiple sclerosis is a chronic autoimmune disease that affects the myelin sheath of nerve fibers in the brain and spinal cord. It is characterized by a large number of symptoms and depends on the level of damage: muscle strength often decreases, reflexes fade, and paralysis (immobility) of various localizations appears.
- Hairy leukoplakia - white areas with a rough surface appear on the mucous membrane of the tongue on the sides, back or lower part. They are painless and do not cause significant discomfort. The main danger lies in the possibility of malignancy of the altered mucosal cells.
- Nasopharyngeal carcinoma is a malignant tumor of the pharynx. Its symptoms often include nasal congestion, hearing loss, frequent ear infections, the appearance of blood in saliva, bloody discharge from the nose, enlarged lymph nodes, and headaches.
- Autoimmune thyroiditis is a chronic disease of the thyroid gland in which antibodies to the thyroid tissue are formed in the body. With this disease, a goiter (enlarged thyroid gland) may appear, and symptoms of hypothyroidism may develop: swelling, increased fatigue, drowsiness, constipation, dry skin, hair loss.
Diagnosis of Epstein-Barr virus
Diagnosis of EBV, regardless of the form of the disease, should be carried out taking into account the epidemiological history, clinical picture and results of laboratory examination.
Laboratory examination includes:
- Epstein-Barr virus, determination of DNA in blood (Epstein Barr virus, DNA);
Epstein Barr Virus nuclear antigen (EBNA), IgG (quantitative)
Anti-EBNA IgG are specific immunoglobulins that indicate past or chronic infection caused by the Epstein-Barr virus.
Synonyms Russian
IgG class antibodies to Epstein-Barr virus JA, class G immunoglobulins to the infectious mononucleosis virus nuclear antigen, IgG class anti-EBNA, IgG-EBNA antibodies.
English synonyms
EBV-NA Antibodies, IgG, Antibodies to Epstein-Barr Virus Nuclear Antigen, IgG, EBNA Antibodies, IgG, EBNA-IgG Ab.
Research method
Enzyme-linked immunosorbent assay (ELISA).
What biomaterial can be used for research?
Venous, capillary blood.
How to properly prepare for research?
Do not smoke for 30 minutes before the test.
General information about the study
Epstein-Barr virus belongs to group 4 human herpes viruses. It tends to attack B lymphocytes and causes an acute disease in humans - infectious mononucleosis, and is also associated with the development of nasopharyngeal carcinoma, Burkitt's lymphoma, Hodgkin's disease, hairy leukoplakia and B-cell lymphoma.
The virus is spread all over the world. In some countries, up to 95% of the population aged 40 years has been previously infected with it and has antibodies. The infection is transmitted through saliva. The peak incidence is observed in early childhood, as well as in adolescence.
Through the epithelium of the mouth, throat and salivary glands, the virus enters the bloodstream and penetrates B-lymphocytes, stimulating their reproduction. As a result, the tonsils, lymph nodes, and spleen enlarge. With normal cellular immunity, infected B lymphocytes and the virus are cleared from the blood and the symptoms of the disease gradually disappear. Epstein-Barr virus, like other herpes viruses, is capable of becoming a latent infection. Its genetic material may be retained in a small number of B lymphocytes and is capable of asymptomatic reactivation. With defects in cellular immunity, HIV, and immunosuppressive therapy, the Epstein-Barr virus is dangerous for cancer (for example, B-cell lymphoma, nasopharyngeal carcinoma).
In many cases, the primary infection is asymptomatic or with moderate pharyngitis and tonsillitis. Symptoms of infectious mononucleosis appear in 35-50% of infected people.
The incubation period of the disease is 4-6 weeks. During the prodromal period, the infection is manifested by muscle pain, fatigue, and general malaise. Then comes fever, sore throat, enlarged lymph nodes, spleen and sometimes liver. In some cases, a rash appears on the arms and torso. Symptoms persist for 2-4 weeks.
With the onset of symptoms, atypical mononuclear cells (> 10% of lymphocytes) and indicators of liver dysfunction are detected in the blood.
The main antigens of the Epstein-Barr virus, to which antibodies are determined: viral capsid antigen (VCA), early antigen (EA) and nuclear antigen (EBNA).
EBNA antigens are found in the nuclei of all cells modified by the Epstein–Barr virus. They are found in tumor cells from Burkitt's lymphoma and nasopharyngeal carcinoma. Anti-EBNA antibodies are rarely present in the blood during acute infection, increasing during recovery from infectious mononucleosis and then reaching a stable level after 3-12 months. In the blood, antibodies to the nuclear antigen of the virus are detected on average 2-4 months after the disease and can persist throughout life.
The absence of anti-EBNA with positive anti-VCA class IgM indicates primary infection with the Epstein–Barr virus. Elevated IgG titers to the capsid antigen in the absence of anti-EBNA 4 weeks after the first symptoms of the disease also indicate a primary infection.
If anti-EBNA is positive, an increase in anti-EA levels may be associated with an exacerbation of latent infection. However, the simultaneous presence of these immunoglobulins in the blood does not always indicate a connection between the patient’s condition at the time of examination and the Epstein-Barr virus. This is because antibodies can be detected for several years after an infection, and the virus sometimes reactivates without any symptoms.
Diagnosis of infection caused by the Epstein-Barr virus cannot be based only on an increased amount of anti-EBNA IgG antibodies, since they can also be detected in healthy people who have previously had infectious mononucleosis.
Simultaneous determination of antibodies to early antigens, capsid protein, and nuclear antigens allows the identification of Epstein-Barr virus infection and determine whether it is current, recent, or long-standing.
What is the research used for?
- For the diagnosis of infectious mononucleosis.
- For differential diagnosis of diseases whose symptoms are similar to infectious mononucleosis.
- To detect exacerbation of chronic infection caused by the Epstein-Barr virus.
- For monitoring certain cancers (Burkitt's lymphoma, nasopharyngeal carcinoma) associated with the Epstein-Barr virus.
When is the study scheduled?
- For symptoms of infectious mononucleosis (sore throat, enlarged lymph nodes, spleen and liver, fever, fatigue).
- If you suspect a previous infectious mononucleosis.
- When diagnosing lymphoproliferative and oncological diseases presumably associated with the Epstein-Barr virus.
What do the results mean?
Reference values
Result: negative.
If the result is positive, a quantitative value in cu/ml is given.
Reasons for the positive result:
- infectious mononucleosis (during recovery or later);
- previous infection caused by the Epstein-Barr virus (more than 2-4 months after illness);
- chronic infection caused by the Epstein-Barr virus;
- neoplasms associated with the Epstein–Barr virus (Burkitt's lymphoma, nasopharyngeal carcinoma).
Reasons for negative results:
- absence of Epstein–Barr virus;
- incubation, prodromal or acute period of infectious mononucleosis;
- many years after infectious mononucleosis;
- some immunodeficiencies with impaired antibody formation.
Important Notes
- If the result is questionable, the analysis must be repeated after 10-14 days.
- In the differential diagnosis of lymphadenopathy and diseases similar to infectious mononucleosis, especially in pregnant women, it is recommended to exclude toxoplasmosis, cytomegalovirus infection, HIV and herpes virus type 6.
- To determine the activity and period of infection, it is necessary to simultaneously determine the levels of other antibodies to the Epstein-Barr virus.
Also recommended
- Epstein Barr Virus, DNA [real-time PCR]
- Epstein Barr Virus capsid protein (VCA), IgM
- Epstein Barr Virus early antigens (EA), IgG
- Human Herpes Virus 6, DNA [real-time PCR]
- Cytomegalovirus, IgM
- HIV 1, 2 Ag/Ab Combo (determination of antibodies to HIV types 1 and 2 and p24 antigen)
- Toxoplasma gondii, IgM (quantitative)
- Alanine aminotransferase (ALT)
- Aspartate aminotransferase (AST)
- Total alkaline phosphatase
- Total bilirubin
- Complete blood count (without leukocyte formula and ESR)
- Leukocyte formula
Who orders the study?
Infectious disease specialist, pediatrician, general practitioner, therapist, oncologist.
Literature
- Kishkun A. A. Immunological and serological studies in clinical practice. – M.: LLC MIA, 2006. – 335-345 p.
- Dennis L. Kasper, Eugene Braunwald, Anthony Fauci, Stephen Hauser, Dan Longo, J. Larry Jameson. Harrison's Principles of Internal Medicine. 16th ed. NY: McGraw-Hill; 2005: RUB 2,783
- Fischbach FT, Dunning MB A Manual of Laboratory and Diagnostic Tests, 8th Ed. Lippincott Williams & Wilkins, 2008: 1344 pp.
The test will allow your doctor to:
- Diagnose the acute period of infectious mononucleosis;
- Conduct differential diagnosis of diseases whose symptoms are similar to infectious mononucleosis;
- Assess the stage of current infectious mononucleosis;
- Diagnose malignant Burkitt lymphoma;
- Diagnose malignant nasopharyngeal carcinoma.
The study is recommended for:
- Sore throat;
- Enlarged lymph nodes;
- Enlarged spleen and liver;
- Fever;
- Fatigue;
- Athletes with the above symptoms, as they have an increased risk of splenic rupture due to physical activity.
Method:
Enzyme-linked immunosorbent assay (ELISA).
Material for research:
Blood serum.