Historical excursion
Perhaps this idea was first brought to life by the Danish physiologist Paul Rehberg at the beginning of the 20th century. Initially, Reberg used exogenous creatinine for these purposes, administered intravenously to the patient. Therefore, traditionally, variants of hemorenal tests based on the assessment of creatinine excretion by the kidneys are called the Rehberg test.
However, it later became clear that the concentration of endogenous creatinine in the blood plasma is an almost constant value and does not undergo significant fluctuations. Based on this discovery, the test was modified and intravenous administration of creatinine was abandoned, greatly simplifying the analysis.
Analysis of results

Normal indicators
Based on available data (daily urine volume, creatinine concentration in blood and urine), creatinine clearance, that is, glomerular filtration rate (GFR), is calculated.
Normal creatinine clearance is:
- in men – 95 – 145 ml/min;
- in women – 75 – 115 ml/min.
Thus, on average, the glomerular filtration rate is 90 – 120 ml/min.
The glomerular filtration rate is affected by physical activity, emotional state, drinking regimen, and taking medications.
Conditions in which an increase in creatinine clearance is observed
- nephrosis;
- arterial hypertension;
- diabetes;
- nephrotic syndrome.
Low values
A decrease in glomerular filtration rate is observed with:
- glomerulonephritis;
- nephrosclerosis;
- pyelonephritis;
- cardiovascular failure;
- diarrhea;
- liver failure.
Based on the level of glomerular filtration rate, a conclusion is made about the functional capacity of the kidneys. The lower this indicator, the worse the patient’s situation (Table 3). When the glomerular filtration rate is less than 15 ml/min, they speak of end-stage renal failure.
Table 3. Glomerular filtration rate and stages of chronic kidney disease.
| Characteristic | Glomerular filtration rate |
| Kidney damage with an initial decrease in glomerular filtration rate. | 60 – 89 ml/min |
| Moderate decrease in glomerular filtration rate. | 30 – 59 ml/min |
| Marked decrease in glomerular filtration rate. | 15 – 29 ml/min |
| End-stage renal failure. | Less than 15 ml/min |
In addition to determining the clearance of endogenous creatinine, there are other formulas for calculating the glomerular filtration rate, which have their pros and cons:
- Cockcroft-Gault formula;
- MDRD formula;
- CKD-EPI.
A little math
Assessment of the functional state of the kidneys based on hemoral tests is based on the mathematical model given below.
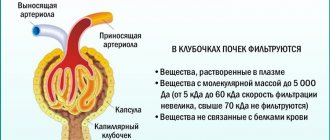
The substance used for the hemorenal test must have the following characteristics:
- the substance used for these purposes is filtered from the blood into the urine by the kidneys
- this substance is not secreted by the kidneys, i.e. all substance enters the urine only as a result of the filtration process
- this substance is not reabsorbed by the renal tubules, i.e. all substances that enter the urine during the filtration process are excreted and do not return to the blood
- an increase in the concentration of a substance in the urine (thickening of urine) occurs only due to the reabsorption of water from it
Substances that have all of the above characteristics are ideal for hemorenal tests, but, unfortunately, they are not found in the human body. Therefore, reference methods are based on intravenous administration of these substances (inulin, 51Cr-EDTA, 125I-iothalamate, iohexol).
As mentioned above, the substance used in the Rehberg test is creatinine, which is the closest marker to the ideal.
Based on these assumptions, the clearance, or purification coefficient, is calculated:
C=UP*Y
Where:
- C - ground clearance
- U is the concentration of the substance in the urine
- P is the concentration of the substance in the blood
- Y—diuresis; the rate of urine production, most often expressed in ml/min.
The physical meaning of clearance: this is the volume of plasma containing the same amount of substance that the kidneys excrete in one minute (the volume of plasma completely cleared of creatinine in one minute).
Based on the fact that the substance appears in the urine only due to filtration and is not reabsorbed, the clearance value is also calculated as the kidney glomerular filtration rate (GFR).
And since the increase in the concentration of the substance occurs due to the reabsorption of water from primary urine, we can also calculate the percentage of water reabsorbed by the kidneys using the formula:
R = F - YF * 100
Where:
- F - glomerular filtration rate
- Y - minute diuresis diuresis
- R is the amount of reabsorption expressed as a percentage
Glomerular filtration rate
Glomerular filtration rate (GFR) is the main indicator of kidney function in healthy and sick people.
Normal GFR for men is 97-137 ml/min, for women - 88-128 ml/min.
Under physiological conditions, GFR increases during pregnancy and when consuming foods high in protein, and decreases as the body ages. Thus, after 40 years, the rate of decline in GFR is 1% per year, or 6.5 ml/min per decade. At the age of 60-80 years, GFR decreases by half. Material from the site https://wiki-med.com
In pathology, the determination of GFR is used to assess the progression of chronic diffuse kidney diseases (chronic glomerulonephritis, amyloidosis, systemic diseases, nephrosclerosis in hypertension, etc.), as well as to assess the effectiveness of therapy.
Calculation of glomerular filtration rate
Glomerular filtration rate (GFR) is calculated using the formula:
F = (Cm / Wed) x V,
where F is the glomerular filtration rate;
Cm—creatinine content in urine;
Cp—plasma creatinine content;
V is the volume of urine excreted in 1 minute (ml).
Clinical use of the Rehberg test
A simplified excretory function of the kidneys looks like this:
Blood flowing through the kidneys enters the nephrons (the smallest functional units of the kidneys), where, under the influence of blood pressure, water and low molecular weight substances are first filtered. The resulting liquid is called primary urine. The amount of primary urine produced per day can reach 150 liters. Next, primary urine enters the convoluted tubule system of the nephron, where the process of concentration occurs due to the reabsorption of water and the formation of secondary urine (normally 1.5 - 2 liters per day). In addition, the reabsorption of a number of filtered low-molecular substances needed by the body (mainly glucose and electrolytes) occurs in the tubules.
Based on the above-mentioned mathematical calculations, using the Rehberg test we can evaluate both filtration (GFR) and concentration (percentage of reabsorption) functions of the kidneys.
Since the glomerular filtration rate depends on the number of functioning nephrons (roughly speaking, on the size of the kidneys), which in turn depends on the “dimensions” of the patient, we get a situation where two absolutely healthy people of different heights and weights can have GFR quite different. Since this would be inconvenient for interpreting the results obtained and determining the reference interval for all combinations of height and weight, another correction factor was introduced to calculate GFR to bring all patients “to a single denominator.” This indicator was the surface area of the human body, which is calculated based on his height and weight. The body surface area was taken as the average statistical value and was equal to 1.73 m2. Thus, when determining GFR, this indicator is usually recalculated accordingly. Decrease if the patient's body surface area is more than 1.73 m2 and increase if less (normalization to the standard body surface area).
The main clinical purpose of performing the Rehberg test is, naturally, to assess kidney function, or rather to determine the number of functioning nephrons, which is the main indicator in making a diagnosis, determining the stage, and also monitoring the dynamics of renal failure.
Selective assessment of reabsorption is performed less frequently and is observed with damage to the distal convoluted tubules of the nephron.
In addition to creatinine, the clearance value in clinical practice is also calculated for some other substances: urea, uric acid (not always for assessing renal function).
Creatinine clearance
Creatinine is the end product of the metabolism of creatine phosphate, a substance involved in quickly meeting the energy needs of muscle contraction; is formed in the muscles and is freely filtered in the glomeruli and then, without being subjected to reabsorption or additional secretion in the tubules, is completely excreted from the body by urine. Therefore, an increase in serum creatinine concentration indicates a decrease in the level of renal filtration (decreased renal function). Reference values for serum creatinine are: for middle-aged men - 62-115 µmol/l, for women - about 53-97 µmol/l. Creatinine formation correlates with muscle mass. Due to the high reserve capacity of renal hemodynamics, creatinine is not a sensitive indicator of kidney disease in the early stages and can remain at a constant level when a significant part of the nephrons is affected. Therefore, it is advisable to simultaneously study serum urea levels.
Currently, in clinical practice it is proposed to abandon the measurement of creatinine clearance. In modern clinical nephrology, calculation methods are used to determine the glomerular filtration rate - the glomerular filtration rate is calculated using serum creatinine concentration and a number of other variables. In this case, the patient’s age, body weight, and serum creatinine concentrations are taken into account.
The MDRD formula (Modification of Diet in Renal Disease; Levey AS et al., 1999) is a study of the effect of dietary changes in kidney disease: GFR, ml/min per 1.73 m2 = (170 x (serum creatinine concentration, mg/ dL - 0.999) x (age - 0.176) x (blood urea nitrogen, mg/dL - 0.170) x (serum albumin, g/dL + 0.318) x (0.762 for women) x (1.18 for African Americans).
Modified MDRD formula: GFR, ml/min per 1.73 m2 = 186.3 x (serum creatinine concentration, mg/dL -1.154) x (age -0.203) x (0.742 for women) x (1.21 for African Americans).
MDRD formula: 186 x blood creatinine (mg/deciliter) - 1.154 x age (in years) - 0.203.
For women, a correction factor of 0.70 is used.
Rules for conducting the Rehberg test
The patient collects urine independently or with the help of health workers for a certain period of time. As a rule, this is a day (1440 minutes), or an option with a two-hour portion of urine (120 minutes). After receiving the last portion, all urine is mixed in one container and the creatinine concentration in it is determined. The value of minute diuresis is obtained by dividing the total volume of urine collected (ml) by the time during which this urine was collected.
On the same day, in the morning on an empty stomach, the patient donates blood to determine serum creatinine.
Next, using the obtained indicators of creatinine concentration in the blood and urine, as well as the weight and height of the patient, GFR and the amount of reabsorption are calculated.
Preparing for analysis

Preparation for the Reberg-Tareev test is the same as for a general clinical urine test. Avoid stressful situations and exhausting physical activity, avoid drinking alcohol, energy drinks, do not consume foods that change the color of urine (beets, carrots), and do not take medications that affect the rate of filtration of the kidneys (diuretics).
Before collecting urine, toilet the external genitalia. Women should not provide urine during their menstrual cycle.
Blood is donated in the morning on an empty stomach. Before the analysis, it is recommended to remain physically and emotionally at rest and refrain from smoking.
How to properly collect urine?

Before you go to donate blood, you need to collect 24-hour urine.
The study of creatinine levels in the blood and daily urine should be carried out on the same day for the reliability of the test results.
Flush the first morning portion of urine into the toilet, and collect all subsequent urinations in a container with a volume of at least 2.5 liters. Urine is stored in the refrigerator. The last portion is one day after the start of collection, that is, the morning portion of the next day.
It is necessary to measure the resulting volume of urine per day, record it and report it to the laboratory. Mix the contents of the container and pour a portion (30 - 50 ml) into a sterile container for analysis, which is sold in a pharmacy. Urine must be delivered to the laboratory as soon as possible; long-term storage will distort the results of creatinine levels.
Disadvantages of the Rehberg test
Currently, the Rehberg test is the most common laboratory test for assessing renal function. But, however, it has a number of significant disadvantages, primarily related to the fact that creatinine is a marker close to ideal only in a certain range of its concentrations. For example, in the later stages of renal failure, GFR may be overestimated due to the fact that blood creatinine, which is in high concentrations, begins to be removed from the body by secretion, and not just by filtration.
In addition, there are certain problems with making a diagnosis in the early stages of renal failure since creatinine has a so-called "blind area". The fact is that due to some compensatory reactions of the body in the initial stages of renal failure, there is no proportionality between the increase in creatinine concentration and the decrease in GFR.
Tubular reabsorption
The Rehberg test allows you to assess the reabsorption function of the kidneys, which is calculated using the following formula: KR (tubular reabsorption) = (GFR - D / GFR) x 100%, where D is minute diuresis. Normally CR = 95-99%. The CR decreases in acute and chronic pyelonephritis, wrinkled kidney, as well as in conditions not associated with kidney disease: taking diuretics, diabetes insipidus.
Categories: Nephrology Urology Excretory system Medical diagnostics Laboratory diagnostics Urine examination
On this page there is material on the following topics:
decreased glomerular filtration according to the Rieberg test
Reberg sample. full height
residual nitrogen Reberg sample
girl's rib test