1.What is a blood calcium test?
A calcium blood test shows the level of calcium in the blood, i.e. that calcium that is not stored in the bones. Calcium is the most abundant mineral in the body and one of the most important. Calcium helps nerves and muscles work, restores bones and teeth, participates in blood clotting and supports heart function.
Typically, the level of calcium in the blood is carefully controlled by the body. If calcium in the blood is low, then the bones give up their calcium to maintain the required level. If the level of calcium in the blood is elevated, then it, on the contrary, penetrates the bones and remains there for storage.
The calcium content in the blood depends on:
- Calcium, which comes to you with food;
- The amount of calcium that the intestines can absorb;
- Various hormones: estrogen, calcitonin and others.
Ionized calcium
Calcium is the most abundant mineral in the human body. The adult human body contains approximately 1 kg of calcium, distributed mainly in the bones in the form of hydroxyapatite. Most of this calcium is stably incorporated into bone, although a small portion is readily exchanged with the soluble fraction of calcium in the body.
Soluble calcium in the body is found primarily in extracellular fluid, with approximately equal concentrations in serum and intercellular fluid. Intracellular calcium concentrations are typically several orders of magnitude lower than extracellular calcium concentrations due to the activity of specific membrane protein pumps, although concentrations within specific intracellular compartments can themselves vary quite markedly. Half of serum calcium exists as a free hydrated cation, slightly less than half is bound to negatively charged amino acid residues on proteins (primarily albumin), and the remainder is complexed with small organic molecules such as lactate and citrate.
Free hydrated divalent calcium cation in serum or plasma has historically been called "ionized calcium" in clinical practice. Although this common description of cationic calcium in solution is accurate, it is incorrect because all calcium in the body is present in ionic form. Non-ionized calcium is a flammable metal that can react violently with water to release hydrogen gas, and is not present in any body tissue.
Calcium homeostasis
Serum proteins, mainly albumin, provide short-term maintenance of a stable concentration of ionized calcium, acting as a calcium buffer. Because ionized calcium is in equilibrium with protein-bound calcium, any short-term drop in ionized calcium concentration can be compensated for by the concomitant release of calcium, in much the same way that weak acids and bases can serve as pH buffers. However, like all calcium buffer systems, albumin-calcium buffer is very sensitive to pH. Changes in pH change the proportion of charged acidic amino acid residues on albumin and thus the amount of bound calcium ions, resulting in a change in the proportion of total free calcium. An isolated increase in pH, such as respiratory alkalosis caused by hyperventilation, causes a fall in ionized calcium, while a decrease in pH, conversely, causes an increase in ionized calcium.
Longer maintenance of a stable concentration of ionized calcium is ensured by the action of several hormones, primarily parathyroid hormone (PTH). Calcium-sensing receptors on the surface of parathyroid cells constantly sense the extracellular concentration of ionized calcium and transmit an intracellular signal that directs the synthesis and secretion of parathyroid hormone when the concentration drops. Parathyroid hormone has effects on several target organs, including the bones, where it directs calcium resorption, and the kidneys, where it increases calcium reabsorption, increases phosphate excretion, and activates 1α-hydroxylase, the enzyme that converts 25-hydroxyvitamin D to its active metabolite . Active metabolite of vitamin D, 1,25-dihydroxyvitamin D, itself
Historically, one of the first published methods for determining ionized calcium was a bioassay that assessed the effect of solutions of varying calcium concentrations on the contractility of the isolated frog heart. Today, several modern methods are used to measure total calcium—dye-calcium complex spectrophotometry, ion selective electrodes (ISE), and atomic absorption spectrophotometry—but ionized calcium is today measured only by direct ISE potentiometry in clinical laboratories. The ISE assay procedure recommended by the International Federation of Clinical Chemistry (IFCC) is described. This procedure uses a reference electrode containing a saturated potassium chloride and a mercury/calomel electrode, and an ISE containing an internal reference solution consisting of calcium and sodium chloride solutions and a standard Ag/AgCl electrode. A liquid membrane containing an organic calcium chelating molecule separates the ISE from the sample so that only calcium cations can pass through the membrane. The calcium chelator used in the membrane is most often a neutral organic molecule dissolved in an organic liquid and polymer matrix, but charged organophosphate chelators such as bis(di-n-octylphenyl) phosphate. The potential that develops across the membrane when measured between the sample and the reference electrode is logarithmically related to the free calcium ion activity in the patient sample. Thus, the concentration of ionized calcium in a patient sample can be mathematically inferred from the measured potential, the calcium concentration in the ISE solution, and the calcium activity coefficients. However, patient results are most often obtained by comparing the measured potential with the potential generated by calibration solutions, that is, with a standard curve. Calibration solutions must be prepared carefully, with a molal ionic strength close to that of normal plasma (approximately 0.160 mol/kg) so that calcium activity coefficients in calibration solutions reflect those in clinical samples.
While no commercial vendor currently offers ionized calcium analysis on a large automated instrument, many of the routine smaller instruments used for blood gas measurement in acute care settings offer direct ISE ionized calcium analysis. The typical reference range for ionized serum calcium from the author's institution, measured on a Roche AVL 9180 analyzer (and validated on several other analyzers since then), is 1.18–1.38 mM in adults. Due to potential preanalytical variability between collections of serum, heparinized whole blood, and heparinized plasma, reference ranges should be verified for these specific sample types.
Ionized hypocalcemia
Ionized hypocalcemia has classic symptoms that include neuromuscular irritability, cramps, tetany, and paresthesia. Clinical signs of the same name include Chvostek's sign (contraction of the facial muscles after tapping the facial nerve) and Trousseau's sign (muscle spasms of the hand and forearm after brachial artery occlusion), both of which reflect neuromuscular excitability associated with hypocalcemia. Circumferential oral paresthesia, which may result from hyperventilation, is also likely due to transient ionized hypocalcemia caused by respiratory alkalosis. Mild ionized hypocalcemia may not cause any symptoms.
Numerous studies over the past few decades have shown that ionized hypocalcemia is common in disease. In some of these studies, the severity of hypocalcemia was directly correlated with disease severity. Another large study of hospitalized patients found that ionized calcium concentrations in patients seemed to be generally distributed around a lower mean value. This finding raises the possibility that calcium is regulated to a lower homeostatic set point during illness, perhaps analogous to the changes in serum protein that are observed during the well-known acute phase response. This view is supported by studies showing that severe hypocalcemia is very difficult to correct with calcium therapy, suggesting that there are concerted physiological mechanisms.
responsible for maintaining low levels of ionized calcium during severe illnesses of many types. However, no study has yet determined what therapeutic strategy, if any, should be taken to counteract ionized hypocalcemia in critically ill patients. Numerous animal studies show that correction of hypocalcemia in animal models of severe disease increases mortality, raising the question of whether ionized hypocalcemia may be beneficial in the disease. There have been no blinded randomized trials comparing calcium monitoring and supplementation with no effect or placebo in hospitalized patients, but a recent review of evidence-based medicine on this topic concluded that there is no evidence that parenteral calcium supplementation affects the outcome of critically ill patients. Despite the high prevalence of ionized hypocalcemia in critical illness and the lack of evidence supporting calcium therapy in unselected patients with critically ill hypocalcemia, there are many specific causes of hypocalcemia that require careful monitoring and treatment. Ionized hypocalcemia is important for monitoring and correction in patients with hypoparathyroidism, the most common cause of which is iatrogenicity after parathyroid resection. Other indications for monitoring and correcting ionized hypocalcemia include acute pancreatitis, extreme vitamin D deficiency, and bone remineralization after surgery for hyperparathyroidism. Intraoperative monitoring of ionized calcium is also warranted in cases of perturbation of homeostasis, such as liver transplantation, and during transfusion of blood products, where significant amounts of the calcium citrate chelator may be delivered at a rate exceeding the metabolic capacity of the liver.
Ionized hypercalcemia.
Ionized hypercalcemia is rarely symptomatic, and when it is, symptoms are quite nonspecific, including fatigue and weakness. Symptoms may also be due to secondary events associated with hypercalcemia, such as kidney stones or osteoporosis. In contrast to ionized hypocalcemia, ionized hypercalcemia is relatively rare in the general inpatient population. When present, it is usually abnormal and merits investigation. Documentation of ionized hypercalcemia should include more than one measurement to ensure that preanalytical factors do not interfere with the analysis. Causes of ionized hypercalcemia include primary hyperparathyroidism, the most common cause of ionized hypercalcemia in outpatients, and malignancy, the most common etiology in hospitalized patients. Additional, less common causes include vitamin D excess, granulomatous disorders, and renal failure. Hypercalcemia associated with malignancy may result from the tumor's secretion of PTH-related peptide (PTHRP), a hormone that can bind to PTH receptors and stimulate bone resorption. Malignancies can also lead to bone resorption due to the direct impact of metastases. Both malignancies and some granulomatous diseases can increase ionized calcium levels by converting 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.
Summary
The ionized calcium test should be considered the most physiologically relevant assessment of calcium homeostasis in humans and, if available, should be used to diagnose calcium disorders in patients. However, with the exception of patients with known or suspected specific disorders of calcium metabolism, it is unclear which patients require calcium monitoring or concomitant therapy. Ionized hypocalcemia is ubiquitous in hospitalized patients, is difficult to correct with calcium therapy, and therapeutic correction of hypocalcemia is of questionable benefit in animal models, indicating that the hypocalcemia observed in up to half of all patients may in fact be a normal and protective response for illness. Therefore, the true value of calcium testing (total, albumin-corrected, or ionized) as a screening tool in unselected patients should be considered unknown. Further research is needed to determine whether a general cycle of screening and calcium supplementation provides any benefit in unselected patients.
2.Why is a blood test done for calcium?
A calcium blood test is done to:
- Check for kidney and parathyroid gland problems;
- Find out the cause of the abnormal ECG;
- Check the condition of the transplanted kidney;
- Check for symptoms of low blood calcium, such as muscle spasms, twitching in the fingers and around the mouth;
- Check for symptoms of high blood calcium levels such as weakness, lack of appetite, nausea, vomiting, constipation, excessive urination, aching bones, abdominal pain.
A calcium blood test cannot tell whether you are getting enough calcium in your diet. For these purposes, it is necessary to check bone density.
Basic comprehensive blood test
To identify osteoporosis at an early stage, the doctor studies the family history (the presence of typical symptoms in relatives), the patient’s complaints, conducts an examination and prescribes laboratory and instrumental examinations. The most informative analyzes are:
- bone destruction indicator deoxypyridinoline;
- osteocalcin, a marker of new bone formation;
- parathyroid hormone;
- estradiol (female sex hormone);
- vitamin D.
Example of blood test results in patients with osteoporosis and degenerative spine diseases
It is important to carry out these tests from January to the end of March, since it is during this period of time that the maximum deficiency of vitamin D and excess parathyroid hormone are detected
Deoxypyridinoline, urine DPID
It is a “bridge” between collagen molecules, transverse connecting threads that give strength to bone tissue. When bones are destroyed, it enters the bloodstream and is excreted in the urine. The analysis shows the rate of bone loss and the risk of fractures. In osteoporosis, an increase in the DPID/creatinine ratio from 5.4 for men and 7.4 for women is found.
High values are also associated with metastasis of tumors to the bones and with a kidney transplant.
Osteocalcin
This protein connects calcium and the main bone mineral, hydroxyapatite. The concentration of osteocalcin in the blood reflects the rate of synthesis of new tissue. Regulates the process of absorption of calcium and phosphorus, the intensity of mineral metabolism. Its content is influenced by vitamin K and D, calcitonin and parathyroid hormone. The normal range is from 4 to 13 ng/ml. Increased in osteoporosis.
Parathyroid hormone
Acts on the kidney tubules, slows down the excretion of calcium, accelerates the release of phosphates. Inhibits the formation of new bone tissue by osteoblasts and activates the destruction of already formed bones. In elderly patients and with osteoporosis, against the background of excess adrenal hormones, parathyroid hormone is increased, and in menopausal metabolic disorders it is decreased. The normal level in the blood is 1.6 to 6.8 pmol/l.
Estradiol
With its deficiency in the body, the sensitivity of bone tissue to the action of parathyroid hormone increases. If the level of female sex hormones from the estrogen group falls below 15-20 ng/ml, then bones begin to rapidly deteriorate in both women and men.
Vitamin D
The main role in the body is to regulate calcium metabolism. With its deficiency, osteoporosis, diabetes mellitus, tumor processes, tuberculosis, and myocardial ischemia progress. Physiological decline occurs in old age and during pregnancy. To prevent osteoporosis, it is necessary to maintain blood levels in the range from 30 to 70 mcg/l.
4.What are the risks and what could interfere with the analysis?
What are the risks of a calcium blood test?
If you are taking a blood test for calcium, then possible risks may only be associated with taking blood from a vein. In particular, the appearance of bruises at the puncture site and inflammation of a vein or artery (phlebitis). Warm compresses several times a day will relieve phlebitis. If you are taking blood thinning medications, you may bleed at the puncture site.
What can affect the results of the analysis?
A calcium blood test may give inaccurate results if:
- You took calcium or vitamin D in any form (not only specially prepared preparations, but also, for example, dairy products) immediately before the test;
- You have had dialysis;
- You recently had a large blood transfusion.
How the level is adjusted
Parathyroid hormone and calicitriol (vitamin D3), as well as calcitonin, are responsible for regulating these processes. Parathyroid hormone and vitamin D3 increase the level of calcium in the blood, and calcitonin, on the contrary, decreases it.
For reference. Calcitriol ensures the absorption of Ca and P in the intestine.
Due to the action of parathyroid hormone:
- ensures an increase in plasma calcium concentration;
- its leaching from bone tissue increases;
- stimulates the conversion of inactive vitamin D into active calcitriol (D3) in the kidneys;
- renal reabsorption of calcium and excretion of phosphorus is ensured.
There is a negative feedback relationship between parathyroid hormone and Ca. That is, when hypocalcemia occurs, the secretion of parathyroid hormone is stimulated, and with hypercalcemia, its secretion, on the contrary, decreases.
Calcitonin, which is its physiological antagonist, is responsible for stimulating the utilization of calcium from the body.
Normal blood calcium levels in women (table)
The norms of calcium in the blood are determined by doctors for each age category. Children's need for macronutrients is 30% higher than adults. Women require more Ca than men. Calcium consumption increases during puberty and pregnancy. According to medical research, only 14% of people get the required amount of calcium from food, the rest are deficient in this element.
Ca is absorbed in the duodenum and small intestine. If a moderate amount of the substance enters the body, then absorption occurs using the receptors of the small intestine; with a large intake of Ca from food, intercellular mechanisms are included in the process, most of it is absorbed by the duodenum.
The normal level of calcium in the blood of women is shown in the table:
| Age | Content in mmol/l |
| Up to 1 month | 1,9-2,55 |
| 1 month - 2 years | 2,25-2,29 |
| 2 years - 14 years | 2,18-2,75 |
| 14 years and older | 2,2-2,6 |
| Pregnant | 2,2-2,7 |
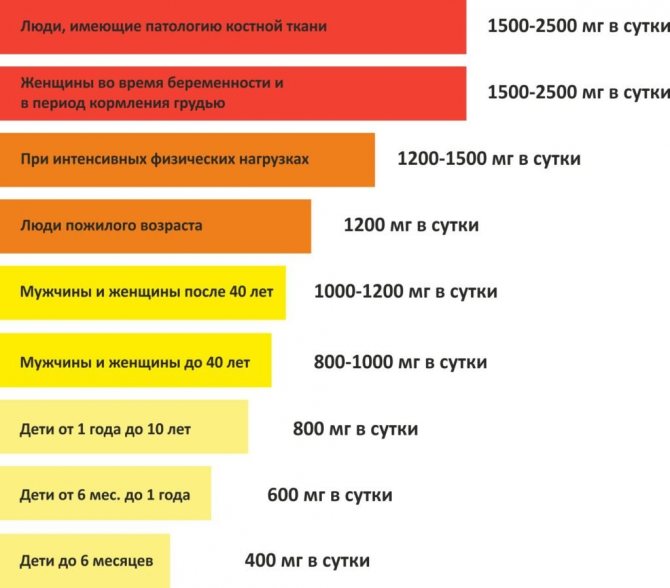
Every day a person should consume 1000 mg of calcium with food; in adolescents and pregnant women this figure increases to 1300 mg. It is important for adolescents to receive the norm due to the intensive growth of the skeleton; in pregnant women, the consumption of macronutrients is increased due to the consumption of calcium by the fetus.
Signs of hypocalcemia. Treatment with food
The main symptoms indicating low calcium levels are drowsiness, confusion, cramps in the feet and hands, and reversible heart failure. In addition, the individual is concerned about:
- headache;
- memory problems;
- numbness of fingers;
- pain in joints and bones;
- pressure changes;
- epigastric pain;
- brittle nails;
- caries;
- periodontal disease.

To raise your calcium levels, it is recommended to adjust your diet to include:
- dairy products;
- dried fruits;
- fish;
- nuts;
- legumes;
- vegetable oils;
- fruit juices;
- chocolate;
- cocoa;
- cabbage;
- bread with bran.
Additionally, the doctor will prescribe medications containing this element.