Follicle-stimulating hormone, designated by the English term FSH, is a gonadotropin consisting of more than two hundred amino acids. This hormone is secreted by the pituitary gland. In a woman’s body, the secretion of hormones depends on age and the phase of the menstrual cycle, so FSH norms vary.
In the female body, follicle-stimulating hormone is responsible, among other things, for stimulating the synthesis of estrogen and the production of progesterone. It is also a factor responsible for egg production and follicle maturation.
FSH hormone - study in women
The content of the article
For women, tests for follicle-stimulating hormone levels are recommended in several cases. Most often, diagnosis is associated with infertility treatment, since the test helps determine a woman's ovarian reserve.
Other diseases that require FSH testing include:
- pituitary gland abnormalities (both sexes);
- menstrual irregularities;
- hypergonadism.
The test may also be given to children who experience puberty too early or too late, which may be due to problems with certain areas of the brain.
FSH levels are also measured in perimenopausal women. Interestingly, research is still ongoing into the possibility of using follicle-stimulating hormone taken from women during menopause to treat younger women who are struggling with infertility. The administration of the hormone should stimulate ovulation and thus increase the likelihood of fertilization during ovulation.
Testing follicle-stimulating hormone levels can also be useful in diagnosing a number of other women's conditions, including polycystic ovary syndrome.
Polycystic ovary syndrome
Follicle stimulating hormone (FSH)
Follicle-stimulating hormone (FSH) is a glycoprotein hormone that is produced and accumulated in the anterior pituitary gland and affects the functioning of the gonads.
Synonyms Russian
FSH, follitropin, pituitary gonadotropin.
English synonyms
Follicle-Stimulating Hormone, Follitropin, FSH, Pituitary Gonadotropin.
Research method
Chemiluminescent immunoassay.
Units
mIU/ml (international milliunit per milliliter).
Determination range: 0.1 - 200 mIU/ml.
What biomaterial can be used for research?
Venous blood.
How to properly prepare for research?
- Do not eat for 2-3 hours before the test (you can drink clean still water).
- 48 hours before the study (in consultation with the doctor), stop taking steroid and thyroid hormones.
- Avoid physical and emotional stress 24 hours before the test.
- Do not smoke for 3 hours before the test.
General information about the study
Follicle-stimulating hormone (FSH) together with luteinizing hormone (LH) is produced in the anterior pituitary gland under the influence of hypothalamic gonadotropin-liberating hormone. FSH secretion occurs in pulse mode at intervals of 1-4 hours. During a surge lasting about 15 minutes, the concentration of FSH exceeds the average by 1.5-2.5 times and is regulated by the level of sex hormones according to the principle of negative feedback. Low levels of sex hormones stimulate the release of FSH into the blood, and high levels inhibit it. The production of FSH is also suppressed by the protein inhibin B, which is synthesized in ovarian cells in women and in the cells lining the seminiferous tubules (Sertoli cells) in men.
In children, FSH levels increase briefly after birth and fall very sharply at 6 months in boys and at 1-2 years in girls. Then it increases before the onset of puberty and the appearance of secondary sexual characteristics. One of the first laboratory indicators of the onset of puberty (puberty) in children is an increase in FSH concentration at night. At the same time, the response of the gonads increases and the level of sex hormones increases.
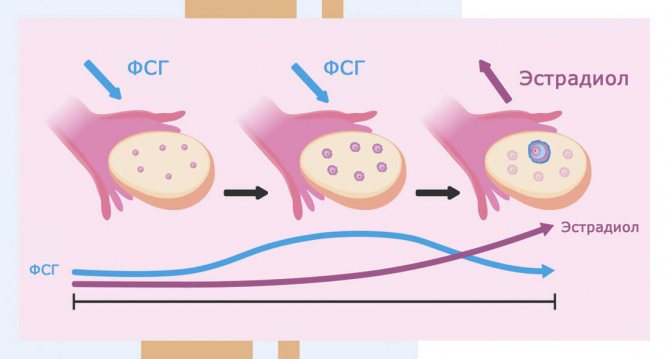
In women, FSH stimulates the maturation of ovarian follicles, prepares them for the effects of luteinizing hormone and enhances the release of estrogens. The menstrual cycle consists of follicular and luteal phases. The first phase of the cycle takes place under the influence of FSH: the follicle enlarges and produces estradiol, and at the end, a sharp increase in the levels of follicle-stimulating and luteinizing hormones provokes ovulation - the rupture of a mature follicle and the release of an egg. Then comes the luteal phase, during which FSH promotes the production of progesterone. Estradiol and progesterone regulate the synthesis of FSH by the pituitary gland via a feedback principle. During menopause, the ovaries stop functioning and decreased secretion of estradiol leads to increased concentrations of follicle-stimulating and luteinizing hormones.
In men, FSH affects the development of seminiferous tubules, increases testosterone concentrations, stimulates the formation and maturation of sperm in the testicles and promotes the production of androgen binding protein. After puberty, FSH levels in men are relatively constant. Primary testicular failure leads to an increase in its number.
Analysis for gonadotropic hormones allows you to determine the level of hormonal regulation disorders - primary (depending on the gonads themselves) or secondary (associated with the hypothalamic-pituitary axis). In patients with testicular (or ovarian) dysfunction, low FSH levels indicate dysfunction of the hypothalamus or pituitary gland. An increase in FSH indicates a primary pathology of the gonads.
Simultaneous tests for follicle-stimulating and luteinizing hormones are used to diagnose male and female infertility and determine treatment tactics.
What is the research used for?
- To identify the causes of infertility (together with a test for other sex hormones: luteinizing hormone, testosterone, estradiol, progesterone).
- To determine the phase of the menstrual cycle (menopause).
- To diagnose the causes of spermatogenesis disorders and reduced sperm count.
- To identify primary or secondary causes of sexual dysfunction (pathology of the gonads or hypothalamic-pituitary disorders).
- For the diagnosis of early or late puberty.
- To monitor the effectiveness of hormone therapy.
When is the study scheduled?
- For infertility.
- If pathology of the pituitary gland and sexual dysfunction are suspected.
- In case of menstrual irregularities (its absence or irregularity).
- When the patient has congenital diseases with chromosomal abnormalities.
- For growth and maturation disorders in children.
- When using hormonal drugs.
What do the results mean?
Reference values
| Floor | Cycle phase | Reference values |
| Male | 1.5 - 12.4 mIU/ml | |
| Female | Menstrual (1-6th day) | 3.5 - 12.5 mIU/ml |
| Folliculin (proliferative) (3-14th day) | 3.5 - 12.5 mIU/ml | |
| Ovulatory (day 13-15) | 4.7 - 21.5 mIU/ml | |
| Luteal (15th day - beginning of menstruation) | 1.7 - 7.7 mIU/ml | |
| Postmenopause | 25.8 - 134.8 mIU/ml | |
| Premenopause | 1.7 - 21.5 mIU/ml |
Menopause. Reasons for increased FSH levels
- Primary ovarian failure (premature ovarian failure syndrome, ovarian dyskinesia syndrome, ovarian tumors and cysts, Shereshevsky-Turner syndrome, Swire syndrome, insufficient production of steroid hormones by the ovaries - 17-alpha-hydroxylase deficiency).
- Primary testicular failure in men (testicular aplasia or agenesis, Klinefelter syndrome, testicular tumors).
- Hypogonadism due to exposure of the ovaries or testicles to any external factors (x-rays, chemotherapy, alcohol, infectious diseases, autoimmune diseases, trauma, castration).
- Hyperfunction or tumors of the pituitary gland.
- Endometriosis.
- Testicular feminization.
- Ectopic secretion in some hormone-secreting neoplasms (usually in lung tumors).
- Premature puberty.
- Alcoholism.
Reasons for decreased FSH levels in the blood
- Deficiency of hypothalamic gonadoliberin (Kallmann syndrome - congenital secondary hypogonadism - a disorder of impulse secretion of gonadoliberin in the hypothalamus).
- Isolated FSH deficiency.
- Pituitary insufficiency.
- Dwarfism.
- Sheehan's syndrome.
- Hyperprolactinemia.
- Neoplasms of the ovaries, testes and adrenal glands with increased secretion of estrogens and androgens.
- Polycystic ovary syndrome.
- Hemochromatosis.
- Anorexia and starvation.
What can influence the result?
- Inadequate FSH levels are possible due to the patient taking radioisotope drugs, oral hormonal drugs, pregnancy, introduction of heterophile antibodies (including monoclonal) into the body, nuclear magnetic resonance scanning of the patient performed shortly before the FSH test, smoking and alcohol consumption.
- Medicines and substances that increase the level of FSH in the blood: bicalutamide, bromocriptine, cimetidine, clomiphene, danazol, digitalis, erythropoietin, finasteride, GnRH analogs, somatoliberin, hydrocortisone, ketoconazole, leuprolide, levodopa, metformin, naloxone, nilutamide, phenytoin, pravastatin, tamoxifen.
- Medicines and substances that reduce the level of FSH in the blood: anabolic steroids, anticonvulsants, carbamazepine, conjugated estrogens, corticoliberin, danazol, diethylstilbestrol, estrogen- and progesterone-containing drugs, finasteril, goserelin, medroxyprogesterone, megestrol, octreotide, oral contraceptives, phenothiazides, pimozide, prednisolone, stanozolol, toremifene, valproic acid.
Important Notes
- In women, the FSH test should be carried out taking into account the day of the menstrual cycle. FSH concentrations peak during ovulation, so the test is usually taken on days 6-7 of the cycle or as directed by your doctor.
- If FSH is low, it is necessary to donate blood again, since the release of the hormone from the pituitary gland is pulsed and one-time testing may not reflect the actual activity of hormonal regulation. At the same time, in conditions associated with an increase in FSH, a single sample is considered sufficient.
- Patients receiving biotin in high doses (> 5 mg/day) can only be tested if more than eight hours have passed since taking the drug.
- FSH levels increase with age.
Also recommended
- Luteinizing hormone (LH)
- Estradiol
- Progesterone
- Testosterone
- Testosterone free
- Sex hormone binding globulin (SHBG)
- Prolactin
- Dihydrotestosterone
- Dehydroepiandrosterone sulfate (DEA-SO4)
- Inhibin B
- Anti-Mullerian hormone
- Androstenedione
- Spermogram
- Thyroid-stimulating hormone (TSH)
- Adrenocorticotropic hormone (ACTH)
- Somatotropic hormone
Who orders the study?
Endocrinologist, obstetrician-gynecologist, pediatrician, andrologist, reproductive specialist.
Literature
- Fischbach FT, Dunning MB A Manual of Laboratory and Diagnostic Tests, 8th Ed. Lippincott Williams & Wilkins, 2008: 1344 pp.
- Fisher DA The Quest diagnostics manual. Endocrinology test selection and interpretation, 4th ed. San Juan Capistrano, CA: Quest Diagnostics Nichols Institute, 2007:369 pp.
- Wilson D. McGraw-Hill Manual of Laboratory and Diagnostic Tests 1st Ed Normal, Illinois, 2007:366 pp.
FSH hormone is the norm for women, men and children
In women, unlike men, there are several norms of this hormone, since in different phases of the menstrual cycle its level has different values. For individual phases in women, the following norms of follicle-stimulating hormone are indicated:
- less than 12 IU/l in the follicular phase;
- from 20 to 90 IU/l during ovulation;
- less than 10 IU/l in the luteal phase.
Changes in FSH levels during the menstrual cycle
FSH levels also change during periods characterized by significant changes in the endocrine sphere. For example, in menopause, this is a level in the range from 40 to 250 IU/l. In the future, the concentration of this hormone in the blood may increase even more. And in case of pregnancy, the woman’s body must contain a small amount of follicle-stimulating hormone.
For men, a single norm has been established for follicle-stimulating hormone - between 4 and 25 IU/l.
As mentioned above, sometimes follicle-stimulating hormone levels are also measured in children. The FSH standard for children under eleven years of age is less than 2 IU/L.
If a test for FSH levels was prescribed due to infertility, it is recommended to simultaneously test for lutropin. This is important, since the ratio of lutropin (indicated by the symbol LH) to the FSH hormone is of great importance in the diagnosis of infertility.
Hormone functions
In the female and male body, the PS hormone plays a different role. In women without FSH, normal egg maturation is impossible. The maturation of the oocyte (sex cell) in the dominant follicle (tissue fragment in the ovary) occurs under the influence of follitropin. The follicle matures, bursts and releases the egg at a maximum concentration of follicle-stimulating hormone around the middle of the cycle.
The FSH hormone, together with LH, stimulates the production of estrogens and, in particular, estradiol and progesterone in the luteal phase, promotes the conversion of testosterone (sexual male androgen) into estradiol, controls the menstrual cycle with other hormonal substances, and affects the health of the female reproductive organs.
In men, testosterone is produced under the influence of follitropin, which promotes the growth of tubules, the formation of viable “fast” sperm, the development of male reproductive organs, sexual desire, and normal spermatogenesis.
What does high FSH mean?
Testing follicle-stimulating hormone levels is important for diagnosing many diseases. High levels of this hormone in women can indicate primary ovarian failure, ovarian tumors, thyroid problems, adrenal disease, Turner syndrome and polycystic ovary syndrome, among other things.
High FSH levels can also occur during chemotherapy and radiation. This is also characteristic of the menopausal condition in women.
In men, high levels of follicle-stimulating hormone may indicate testicular failure, leading to infertility. In addition, levels that are too high may indicate hypogonadism, especially in Klinefelter's syndrome and testicular infections of various origins, which can also affect sperm production and therefore cause male sterility.
ONLINE REGISTRATION at the DIANA clinic
You can sign up by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
If you find an error, please select a piece of text and press Ctrl+Enter
Follicular phase of the menstrual cycle
The follicular phase is so named because during this period several follicles begin to develop. To initiate the follicular phase, the pituitary gland secretes the FSH hormone.
Around day 6–7 of the follicular phase, one follicle is released and continues to grow and develop. Within about two weeks, an egg matures in it, which must be fertilized by a sperm.
From the beginning of the follicular phase until the ovulation phase, the amount of estrogen gradually increases. The follicular phase ends. If for women it takes 28 days from the first day of menstruation to the start of the next menstruation, then the follicular phase lasts 14 days. If the menstrual period is longer, then the follicular phase of the cycle occurs later.
FSH: normal
In laboratories, the hormones LH and FSH are measured in international units per liter. You need to be tested for FSH, prolactin, LH and other hormones on an empty stomach. An analysis for follicle-stimulating hormone is taken on the 3rd–5th day of the cycle (follicular phase period).
Normal for women
The FSH norm in women varies throughout the menstrual cycle:
follicular phase of the cycle - 2.8–11.3 mU/l;
ovulatory phase of the cycle - 5.8–21 mU/l;
luteal phase of the cycle - 1.2–9 mU/l.
Normal for men
Normal FSH levels in men should be between 1.37 and 13.58 mU/L. If FSH levels are low, the child may experience delayed puberty.
If the analysis shows an insufficient amount of this hormone in a woman, the following symptoms may occur:
- scanty periods;
- lack of ovulation;
- infertility;
- atrophy of the mammary glands and genital organs.
The reasons for reduced FSH levels in women may be obesity and polycystic ovary syndrome, as well as disorders in the hypothalamus.
Low FSH in men indicates:
- impotence;
- lack of sperm in semen;
- testicular atrophy.
In men, low levels of this hormone may be due to insufficient function of the pituitary gland.
With low FSH levels, both men and women experience decreased libido, decreased body hair growth (secondary sexual characteristics), and wrinkled skin.
High FSH
When FSH is elevated, women may:
- uterine bleeding not associated with menstruation occurs;
- no menstruation.
Elevated FSH is normal in women during menopause.
Causes:
- ovarian failure;
- pituitary tumor;
- alcoholism;
- endometrioid cysts;
- exposure to x-rays.
A man may have increased FSH with:
- impaired functioning of the gonads (including inflammation of the testicles);
- increased amount of male hormones;
- X-ray irradiation;
- renal failure;
- alcoholism;
- pituitary tumors;
- taking certain medications.
Reasons for increased FSH
Any hormonal imbalance is fraught with health consequences. To restore the balance of hormones, you need to know the reasons for deviations from the norm. The cause of increased FSH for both sexes can be benign and malignant pituitary tumors, a metastatic process.
Other common reasons include:
- Radiation exposure.
- Alcohol abuse.
- Tobacco smoking.
- Taking certain medications, hormone therapy.
- Oral contraception.
- Renal decompensated failure.
- Anomalies in the development of the gonads and/or pituitary gland.
- Chromosomal mutations (Shereshevsky-Turner syndrome).
In women, follicle-stimulating hormone is increased with cycle disorders, early menopause and menopause, after oophorectomy (removal of the ovaries), depletion of ovarian function, multiple gonadal cysts, and increased testosterone. In men, FSH is increased after orchiectomy (removal of the testicles), with inflammation of the testicles.
LH/FSH ratio: normal in women
The main indicator of the normal function of a woman’s reproductive system is the ratio of the hormones FSH and LH in the body. Before the onset of menarche, this value should be 1. One year after the establishment of regular menstruation, the LH/FSH norm in women can vary from 1 to 1.5. Two years after menarche and before a woman enters menopause, the ratio of FSH and LH in the female body should be from 1.5 to 2. If the level of FSH or LH deviates from the norm, this ratio is changed.
Rules for preparing for FSH analysis
Before taking blood to determine FSH levels, it is recommended to adhere to the following rules:
- one day before the study, you must stop drinking alcohol;
- avoid physical overexertion;
- do not smoke for 1-2 hours before the analysis;
- Blood tests should be performed on an empty stomach.
To analyze the level of FSH in the blood, you must choose a laboratory that is equipped with the latest equipment that meets international diagnostic standards.
The IVF Center clinic in Yekaterinburg specializes in the diagnosis and treatment of pathologies of the reproductive function of men and women. Here tests are carried out to determine the level of hormones in the body. Qualified specialists of the IVF Center will interpret the results of the study in detail and clearly and, thanks to their vast practical experience and individual approach to each patient, will prescribe the optimal treatment tactics for the identified pathologies.
You can make an appointment for tests and consultation with a doctor by phone or on the clinic’s website. Don't waste precious time, take the first step towards your health!