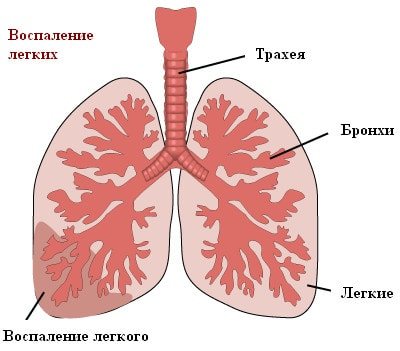
What is pneumonia?
Pneumonia, popularly called “pneumonia,” is damage to the lung tissue. Depending on the stage of the disease, it can affect the lining of the lung and various parts, including the diaphragmatic pleura. Pneumonia is a very dangerous disease, often leading to death, so if there are signs of the disease, doctors prescribe an x-ray.
Causes of the disease
In most cases, pneumonia occurs due to harmful microorganisms entering the organ: viruses, bacteria, fungi. Infection occurs by airborne droplets. Another type, eosinophilic pneumonia, is allergic in nature and requires urgent X-ray examination. Much less often, pneumonia is congestive, for example, when it occurs as a result of prolonged bed rest. It can also be a complication of other diseases. What pneumonia looks like on an X-ray largely depends on the nature and stage of the disease.
Signs of illness
Symptoms of pneumonia do not take long to appear, manifested by a dry or wet cough, with a temperature of up to 40 degrees. With a wet cough, the doctor pays attention to the nature of the sputum: “rusty”, bloody with pus, the presence or absence of odor. Other signs of pneumonia include pain in the chest, side, and even stomach—in this case, an x-ray is needed to confirm the location of the lesions in the lung.
Clinical tests and tasks
1. A 55-year-old patient was found to have a lag in the right half of the chest during breathing, dullness below the level of the 3rd rib, weakened breathing and bronchophony there. X-ray shows a displacement of the heart to the left. Probable diagnosis:
a) exudative pleurisy;
b) lobar pneumonia; c) atelectasis; d) pneumocirrhosis; d) pneumothorax. 2. The asthmatic condition is characterized by all the signs except:
a) impaired consciousness; b) polypnea; c) copious sputum; d) reducing respiratory sounds; e) signs of acute cor pulmonale.
3. The patient's chest movements are symmetrical, with percussion there is a boxy sound, weakened vesicular breathing with prolonged exhalation, hepatic dullness is displaced downward. Your diagnosis:
a) hydropneumothorax; b) fibrosis; c) diffuse pulmonary emphysema; d) bronchial asthma; e) lobular pneumonia.
4. The patient has a normal-shaped chest, no mediastinal displacement, dull sound on percussion, ringing moist rales and distinct crepitus. Your diagnosis:
a) lobar pneumonia; b) emphysema; c) pneumothorax; d) bronchiectasis; e) pulmonary fibrosis.
5. After a breakthrough of an acute single abscess into the bronchus, the following symptoms are usually observed, except:
a) identifying a cavity with a horizontal level on an x-ray; b) increase in body temperature to 39°C and above; c) cough with the release of large amounts of sputum with an unpleasant odor; d) improvement of general condition; d) hemoptysis.
6. Specify the main (constant) diagnostic sign of acute pneumonia:
a) dullness of sound; b) bronchial breathing in the place of dullness of sound; c) fever; d) moist, sonorous fine bubbling rales; e) weakening of breathing.
7. Specify the main radiological sign of lobar pneumonia:
a) homogeneous darkening according to the lobe or segment; b) picture of atelectasis; c) heavy pulmonary pattern; d) focal shadows; e) diffuse decrease in transparency.
8. Moist rales in the lungs are usually heard when:
a) pneumothorax; b) fibrosing alveolitis; c) pleural effusion; d) lung cancer: e) pulmonary emphysema.
9. With chronic obstructive pulmonary diseases, all complications are possible, except:
a) right ventricular failure; b) erythrocytosis; c) respiratory failure; d) left ventricular failure; e) bronchogenic cancer.
10. Restrictive respiratory failure can be caused by the following diseases, except:
a) kyphoscoliosis; b) fibrosing alveolitis; c) obesity; d) laryngeal stenosis; e) exudative pleurisy.
11. The main early sign of peripheral lung cancer:
a) pain in the chest; b) hemoptysis; c) anemia; d) recurrent pneumothorax; d) a dark spot with uneven contours.
12. Which factor is not involved in the mechanism of suffocation in bronchial asthma:
a) alveolar edema? b) swelling of the bronchial mucosa; c) bronchospasm; d) increased secretion of mucus; e) impaired sputum production.
13. All signs are characteristic of bronchial obstruction, except:
a) sputum retention; b) laryngospasm; c) inflammation of the bronchi; d) bronchospasm; e) swelling of the mucous membrane.
14. Which indicator best indicates bronchial obstruction?
a) diffusivity (CO2); b) residual lung volume; c) maximum ventilation of the lungs; d) Tiffno test; e) vital capacity of the lungs.
15. Specify the indications for diagnostic pleural puncture:
a) persistent effusion; b) suspicion of pleural empyema; c) suspicion of cancer etiology; d) unclear causes of effusion; e) in all of the above cases.
16. Chronic obstructive bronchitis is characterized by all the signs except:
a) box percussion sound; b) prolonged exhalation; c) scattered dry wheezing on exhalation; d) bronchial breathing; e) expiratory dyspnea.
17. A 23-year-old man, in perfect health, after a strong cough, experienced an attack of sharp pain in the chest on the right. On examination: tympanitis on the right, decreased breathing and bronchophony. Probable diagnosis:
a) lobar pneumonia; b) acute bronchitis; c) pleurisy; d) pulmonary embolism; e) spontaneous pneumothorax.
18. What sign is not typical for acute lung abscess?
a) hectic fever; b) a thin-walled cavity without a liquid level; c) elastic fibers in sputum; d) neutrophilic leukocytosis; d) blood in the sputum.
19. A patient with chronic cor pulmonale may exhibit all the signs except:
a) shortness of breath; b) tachycardia; c) acrocyanosis; d) right bundle branch block; e) barrel-shaped chest.
Answers 1 – a. 2 – c. 3 – c. 4 – a. 5 B. 6 – d. 7 – a. 8 – b. 9 – d. 10 – d. 11 – d. 12 – a. 13 – b. 14 – d. 15 – d. 16 – d. 17 – d. 18 – b. 19th century
TASKS Task No. 1 Patient K., 22 years old. She was admitted to the hospital with complaints of asthma attacks up to 3–5 times a day (including at night), paroxysmal cough with difficult to clear sputum, shortness of breath with slight physical exertion, and nasal congestion. Suffering from polypous rhinosinusitis since the age of 18. Over the course of 5 years, with a certain cyclicity (in May - June), he notes the appearance of lacrimation, nasal congestion, and difficulty breathing. A history of allergic reactions to taking metamizole sodium was noted: nasal congestion, difficulty breathing. The patient's condition is moderate, respiratory rate (RR) is 22/min. Nasal breathing is severely difficult. Diffuse “warm” cyanosis is noted. On percussion of the lungs there is a boxy sound; on auscultation a large number of dry wheezing sounds are heard on exhalation. Heart rate (HR) – 96/min. Blood pressure – 110/70 mm Hg. Art. Heart sounds are rhythmic and muffled. Clinical blood test: hemoglobin – 128 g/l; erythrocytes – 4.5x1012, leukocytes – 8.0x109; segmented – 63%; lymphocytes – 21%; eosinophils – 13%; monocytes – 3%, ESR – 10 mm/h. General sputum analysis: viscous consistency, mucous character, leukocytes - 1–5 in the field of view; eosinophils – 40–60 in the field of view, Kurshman spirals, Charcot-Leyden crystals. Spirogram: vital lung capacity – 84%; forced expiratory volume in 1st s (FEV1) – 55%; maximum volumetric air velocity at the level of 25% of the forced vital capacity of the lungs (MOC 25) – 66%; MOS 50 – 42%; MOS 75 – 38%. After inhalation of 400 mcg of salbutamol: FEV1 – 84%; MOS 25 – 68%; MOS 50 – 59%; MOS 75 – 58%. An X-ray examination of the chest organs did not reveal focal or infiltrative changes; a flattening of the dome of the diaphragm and an increase in the airiness of the lung tissue were determined. Formulate a clinical diagnosis.
Task No. 2 Patient M., 66 years old. He was admitted to the clinic with complaints of a cough with yellow-green sputum, an increase in body temperature to 38.8oC, shortness of breath with moderate physical activity, pain in the left half of the chest, aggravated by coughing and deep inspiration, general weakness, sweating. I became acutely ill 3 days ago after hypothermia. I took acetylsalicylic acid and bromhexine on my own, but my health did not improve. From the anamnesis it is known that the patient has been smoking 1–1.5 packs of cigarettes per day for 20 years. The general condition is moderate, the skin is clean. Body temperature – 37.6°C. There is no edema, peripheral lymph nodes are not enlarged. RR at rest – 22/min. The chest is emphysematous, there is a lag of its left half during breathing. Percussion - boxed sound, on the left below the angle of the scapula - dullness, in the same place - increased vocal tremors. On auscultation, dry buzzing rales are heard on exhalation; crepitus is heard on the left at the angle of the scapula. Heart sounds are muffled, heart rate – 102/min, blood pressure – 118/76 mm Hg. Art. The abdomen is soft and painless. The liver and spleen are not enlarged. There is no dysuria. Blood tests: hemoglobin – 152 g/l; red blood cells – 5.2x1012; leukocytes – 12.6x109; stab - 4%; segmented – 70%; lymphocytes – 18%; eosinophils – 2%; monocytes – 6%; ESR – 34 mm/h. General analysis of sputum: mucopurulent in nature, leukocytes - completely; acid-fast mycobacteria were not detected; Gram-positive diplococci are determined. An x-ray of the chest organs in 2 projections shows an area of pulmonary tissue infiltration in the lower lobe of the left lung, pulmonary emphysema. Formulate a preliminary diagnosis.
Answers Task No. 1. Bronchial asthma, mixed form (atopic, aspirin-induced), newly identified, severe. Respiratory failure (RF) grades I–II. Polypous rhinosinusopathy. Hay fever with manifestations of allergic rhinoconjunctivitis.
Task No. 2. Community-acquired pneumonia localized in the lower lobe of the left lung, moderate severity, peak phase. Chronic obstructive pulmonary disease, mixed type, moderate severity, DN I-II degrees.
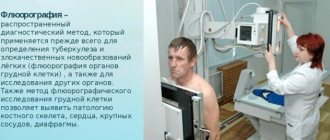
How is an x-ray taken for pneumonia?
For pneumonia, an X-ray of the lungs is usually taken, regardless of the cause of the disease. Before the study, it is necessary to remove everything that could distort the results: metal objects, jewelry, long hair, etc. X-ray of the lungs
done in a vertical position, having first undressed to the waist and stood in front of the machine as the radiologist says. At the doctor’s command, the patient draws air into his lungs and holds his breath, while the device takes a picture.
What does pneumonia look like on an x-ray?
What pneumonia looks like on an X-ray depends on the stage of the disease and its nature. However, in any case, signs of pneumonia on x-ray are visible as disturbances in the structure of the lung. Doctors pay attention to the features of the pulmonary pattern, the roots of the lung, the pleura and the location of infiltrative foci. Light areas in the image are interpreted as airless.
Krupoznaya
Croupous pneumonia on X-ray is characterized by increased pulmonary pattern and thickening of the root, slight compaction of the pleura, as well as reduced airiness of the lung. The reduction in airiness directly depends on the stage of the disease. This disease looks like medium-intensity shading. Lobar pneumonia is one of the most dangerous.
Focal
As with lobar pneumonia, with focal pneumonia, X-rays show an increase in the pulmonary pattern and thickening of the root, as well as thickening of the pleura. Such pneumonia is characterized by focal shadows of different sizes with unclear contours. There is also a deformation of the pulmonary pattern, which is very clearly visible on x-ray. It is difficult to identify symptoms of focal pneumonia on X-rays, so only an experienced doctor can diagnose this disease.
Viral
Viral pneumonia is classified as atypical. With the strengthening of the pulmonary pattern and compaction of the pleura in this case, the roots of the lungs do not change. The appearance on x-ray of focal shadows in the lower and middle parts of the lungs with bilateral viral pneumonia confirms the diagnosis. The whole world is aware of the rapid development and danger of this form of the disease, and this is another argument in favor of examining the signs of pneumonia on an X-ray.
Causes of pneumonia
The most common cause of pneumonia is a bacterial infection. In 30-40% of cases, the causative agent of pneumonia is pneumococcus (a type of streptococcal infection). In addition to bacteria, pneumonia can also be caused by viruses, mycoplasmas, and chlamydia.
Typically, the pathogen enters the lungs aerogenously - with inhaled air. But it is also possible for an infection to enter the bloodstream from an already existing source of inflammation (for example, with peritonitis). The penetration of infection through the upper respiratory tract also in most cases occurs progressively - first, a focus of inflammation appears in the nasopharynx or throat, and only then from there the infection “descends” to the lungs. Thus, any viral disease of the upper respiratory tract (ARVI, influenza) can become a trigger for the development of pneumonia, since viral damage creates favorable conditions for the activation of pathogenic bacteria. If you have tracheitis or bronchitis, you must be observed by an experienced doctor in order to prevent or promptly detect the penetration of infection into the lungs themselves.
Factors contributing to the occurrence of pneumonia (pneumonia)
In some cases, the risk of pneumonia increases. Children are the most vulnerable (due to underdeveloped immunity, respiratory muscles, narrower and shorter airways). Also, pneumonia often develops in older people (over 60 years old), this is associated with age-related weakening of the immune system, loss of muscle tone and low mobility.
Factors that increase the risk of pneumonia also include:
- chronic diseases of internal organs (kidneys, heart) in the acute stage;
- oncological diseases;
- endocrine diseases (diabetes mellitus);
- diseases of the central nervous system (including epilepsy);
- weakened immune system;
- constant stress, depression;
- poor nutrition (insufficient consumption of fruits, vegetables, fish, meat);
- hypothermia;
- smoking;
- alcohol abuse.
Contraindications to X-rays
X-rays should not be taken for pregnant women at any stage, as well as for children under 15 years of age. In some cases, the patient's condition may be an obstacle to conducting the study. A patient in a supine position cannot undergo the study due to the inability to assume an upright position. In an inadequate condition, when the patient cannot stand still, signs of pneumonia on an x-ray cannot be recorded properly.
How often can an x-ray be taken for pneumonia?
A confirmed diagnosis is an indication for regular x-ray examinations to monitor the course of the disease. Whether the treatment prescribed by the doctor helps will show what pneumonia looks like on an x-ray. In this regard, many patients are concerned about how often this procedure can be performed without harm to health. After the start of treatment, depending on the type of disease, an x-ray for pneumonia must be done after 6-10 days. If positive dynamics are noticed, treatment continues as it was started. The patient, who is considered to be cured, is subsequently re-examined after 1, 3 and 6 months. With favorable treatment, the patient receives a small dose of radiation, far from acceptable levels. This is possible thanks to the development of medical technologies and protective measures during the procedure.