What is CT coronary angiography of the heart vessels
Diagnostics is a type of computed tomography.
In this case, using a contrast agent and X-ray radiation, the vascular structures of the myocardium are examined. The method is able to determine the degree of patency of the arteries. If it is broken, it will be shown on the tomographic images. The study is prescribed to patients admitted with complaints of pain in the chest area. They are usually symptoms of coronary artery disease. When the vascular lumens narrow due to the deposition of atherosclerotic plaques on the walls, the myocardium experiences a lack of nutrition. Oxygenated blood stops flowing into the heart muscle, and there is a danger of a heart attack (death of part of the muscle tissue). The more the blood flow through the coronary arteries is impaired, the more serious treatment is required. When medications do not cope with the problem, the patient undergoes surgery. Surgical methods of helping the patient are stenting (installation of a frame to expand the vascular bed) and coronary artery bypass grafting (create an additional path bypassing the damaged section of the artery).
FAQ:
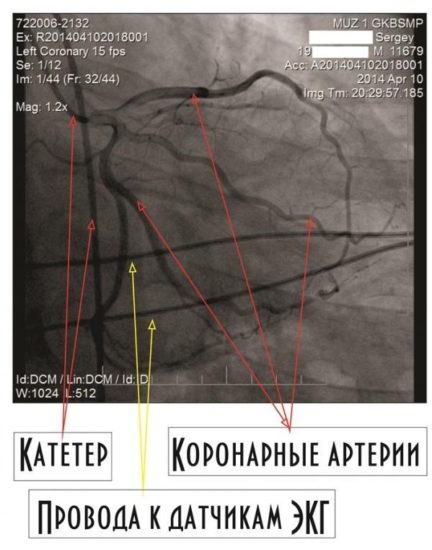
Question: I am 56 years old and have coronary heart disease . The cardiologist recommends a coronary angiography . I don't quite understand what this is? Answer: Coronary angiography is a study of the vessels of the heart, which, like a crown, surround the heart, supplying it with oxygen-rich blood. These are called coronary arteries. Narrowing of the coronary arteries leads to a decrease in blood supply to the heart, which leads to oxygen starvation, i.e. to cardiac ischemia. It is very important to know the condition of the arteries of the heart, because... the obstruction to blood flow can be eliminated, radically relieving the person of the symptoms of coronary heart disease . Question: How is coronary angiography performed? Answer: Coronary angiography is an x-ray examination in which a special contrast agent is injected into the vessels of the heart using a flexible thin probe. As the contrast agent passes through the vessels, short-term x-rays are taken with significant magnification using high-resolution equipment. The slightest changes in the coronary bed are visible “at a glance.” The results are recorded in digital format and are available for viewing on any personal computer. Question: Is coronary angiography performed under anesthesia? Answer: No general anesthesia is required. The pulse is determined in the groin area or on the wrist, and a probe or catheter is inserted into the lumen of the artery under local anesthesia. The subject does not feel how the catheter moves through the vessels, because There are no sensory nerve endings inside the arteries. There is no pain, the patient is fully conscious and, together with the operator, monitors the progress of the study on the monitor. The duration of the procedure is no more than 15-20 minutes. Further monitoring of the patient for several hours is necessary. At the CELT clinic, coronary angiography is performed exclusively through the radial artery (at the wrist). Immediately after the examination, the patient can get up and walk, the bandage on his arm does not limit him in any way (see ambulatory coronary angiography ). After 4 hours the patient is discharged home. If the examination is carried out through the groin, then bed rest is necessary and the period of stay in the clinic is extended to a day. Question: If coronary angiography does not reveal narrowing in the vessels of the heart, then there is no coronary heart disease? Answer: Yes, the absence of changes in the coronary arteries practically excludes the diagnosis of coronary heart disease . In rare cases, ischemia of the heart muscle can occur in the presence of “normal” coronary arteries, but the absence of damage to the arteries of the heart is the most reliable predictor of a good prognosis. This is very important information for choosing the right patient management tactics. Question: At what age is coronary angiography , what are the contraindications to coronary angiography? Answer: Coronary angiography is performed at any age, in all cases when there is a need for it, namely if the patient has angina pectoris after myocardial infarction. Coronary angiography, in the first hours of myocardial infarction , makes it possible to determine where the blockage of the vessel is causing the heart attack and immediately eliminate it. Coronary angiography is necessary for all adults with heart defects before surgery, before “major” vascular operations. Some patients at high risk for coronary heart disease , such as diabetes , may not have symptoms of the disease. In this case, coronary angiography is, in fact, the only reliable way to exclude or confirm coronary disease . Question: I need a coronary angiography . I contacted the Federal Center. They gave me a list of tests and put me on the waiting list. They said I needed hospitalization for 2-3 days. Answer: We coronary angiography on the day of admission! All tests and additional studies are carried out within 4-5 hours, including coronary angiography. Question: How can I get a coronary angiography at your center? Answer: You can come any day, appear at the clinic, at the cardiovascular surgery department in the morning at 08:30 on an empty stomach, PRIORLY AGREEING YOUR ADMISSION WITH US BY PHONE 305-34-04 or 788-33-88. Before admission, before performing coronary angiography , you should have on hand the results of the following tests and studies: - General blood test; — General urine analysis; - Biochemical analysis - protein, urea, creatinine, bilirubin and its fractions, lipid profile, potassium and sodium, glucose; — Coagulogram; — Blood type and Rh factor, Rh antibodies; — Blood test for HIV, RV, antibodies to hepatitis B and C; — Ultrasound of the heart, ECG. If you do not need tests and studies, then they can be performed with us on the day of admission. Question: coronary angiography cost you and what are the prices for coronary angiography in Moscow in other clinics? Answer: Coronary angiography including the stay costs 30,000 rubles. Today, if you analyze the prices for coronary angiography in Moscow, this is the minimum cost.
CT coronary angiography of cardiac vessels and stent installation
Diagnostic clinics only conduct computer scans. Large cardiology and cardiac surgery departments, in addition to this procedure, install a stent when narrowed areas of the artery are detected in a patient. This is a tube whose walls are a metal mesh. It is compressed and supplied using a catheter through the femoral artery to the area with impaired blood flow. Heated by the warmth of the human body, its frame expands and fills the vascular lumen, preventing it from narrowing.
Complications from other organs
Allergic reactions and side effects
Local anesthetics
Allergic and systemic toxic reactions to local anesthetics are very rare. Most often these are skin or vagal reactions, occasionally anaphylactic reactions that pose an immediate threat to life. Very often they are caused by preservatives contained in the drug solution. These reactions can be prevented by using anesthetics without preservatives in the composition.
General anesthesia
In most cases, general anesthesia is not necessary for coronary angiography. However, light sedation and analgesia with short-acting drugs is often used to increase patient comfort and reduce anxiety. In this case, excessive sedation should be avoided, which carries the risk of respiratory arrest or airway obstruction. Constant monitoring of blood pressure, heart rate, respiratory rate and blood oxygen saturation should be carried out in all patients. Anaphylactic reactions to sedative medications are very rare. Treatment for any side effects depends on their severity. To avoid such complications, the patient should tell doctors about his allergies to drugs and food (especially seafood).
Contrast agent

Allergic reaction to contrast agent injection
Adverse reactions to contrast can be divided into toxic and anaphylactic. The toxic and allergic effects of the contrast used depend on its characteristics. New drugs (for example, Visipak) rarely cause mild reactions (feelings of heat, heaviness in the chest, nausea and vomiting), which in most cases go away on their own. More serious complications requiring treatment - drop in blood pressure, bradycardia, pulmonary edema - occur even less frequently. Allergic reactions can manifest as rash, itching, headache, and sometimes anaphylactic shock, Quincke's edema or bronchospasm. To reduce the risk of complications, the patient should inform the doctor about existing allergies to medications, food (especially seafood), asthma or atopic dermatitis.
Heparin-induced thrombocytopenia
This is a serious immunological complication after heparin administration. Because doctors use a heparinized solution when performing coronary angiography, there is a risk of developing this condition. Symptoms of heparin-induced thrombocytopenia occur several days after the procedure. These may include a decrease in platelet count, venous and arterial thrombosis.
Infectious complications
An infectious process can develop at the site of arterial puncture. This complication occurs in less than 1% of patients. Symptoms may include redness at the surgical site, discharge from the wound, and fever. The risk of infection increases if there is a hematoma at the puncture site. To reduce the risk of this complication, the patient should take a hygienic shower or bath before the operation, carefully shave the groin or forearm; For this purpose, it is better to use an electric razor rather than blades, as the latter can leave scratches or cuts on the skin. It is also important that medical personnel working in the operating room strictly adhere to the rules of asepsis and antisepsis. In the postoperative period, water should not be allowed to enter the puncture site during the first 2 days.
Kidney damage
Injection of contrast material, renal artery embolism, or a drop in blood pressure during coronary angiography can cause serious kidney damage. The incidence of renal complications depends on the presence of risk factors (renal failure, diabetes mellitus, old age, use of old high-molar contrast agents) and ranges from 3% to 16%. Fortunately, most patients with this complication have mild, temporary impairment of renal function that usually resolves within a week. In more severe cases, acute and chronic failure may develop, which may require hemodialysis (“artificial kidney”). The incidence and severity of nephropathy depend on the contrast agent used. To prevent the development of this complication, it is necessary that the patient is not dehydrated - that is, he drinks a sufficient amount of water after coronary angiography.
Respiratory failure
Respiratory failure can occur due to many causes, including pulmonary edema due to congestive heart failure and preexisting pulmonary disease, allergic reactions, and excessive sedation.
Advantages of CT coronary angiography of the heart vessels
When performing it, it is not necessary to pierce the artery wall. The puncture is done when CT angiography of the heart vessels is prescribed - its analogue. The puncture requires local anesthesia, since its wall is quite thick. During a CT scan of the coronary system, a contrast agent is administered intravenously. Diagnostics is superior to other methods of examination.
Scanning is considered the “gold standard” in diagnosing IHD. In modern medicine, this is the only research option that helps accurately visualize the anatomical structure of the coronary bed.
Coronary angiography: to do or not to do?
Evgenia, Birsk
August 26, 2016
Hello! My husband (age 40 years, height 174 cm, weight 84 kg) 2 weeks ago was hospitalized in the therapeutic (cardiology) department due to a hypertensive crisis. Complaints: increased blood pressure 180/100, weakness, pain in the heart area radiating to the left shoulder blade, lack of air. Now they diagnose angina pectoris. (See diagnostic results below). The doctor suggests doing a coronary angiography. Now my husband is being treated in a hospital, his condition has improved slightly, there is no pain, slight weakness, and his blood pressure has returned to normal. The first few days I was out of breath, if I walked a little, now I can withstand a small load (calm walking). About 9-10 years ago I was in the hospital with similar symptoms, then they diagnosed a hypertensive crisis. During these 10 years there were slight fluctuations in blood pressure, but overall the condition was normal. Conclusion of ECHO-KG (dated August 12, 2016): Consolidation of the aorta. Hypertrophy of the left ventricular myocardium with a diffuse decrease in contractility. Dilatation of the cavities of both atria. Diastolic dysfunction of the left ventricular myocardium, type 1. Daily monitoring of ECG and blood pressure (from August 9, 2016): bradycardia during the observation period, pronounced during the day. Circadian index 113%. During the observation period, submaximal heart rate was not achieved (48% of the maximum possible for a given age). The dynamics of blood pressure are characteristic of stable isolated diastolic arterial hypotension during the daytime. The decrease in systolic and diastolic blood pressure at night is insufficient. The variability of diastolic blood pressure during the day and systolic blood pressure at night was within normal limits. The variability of systolic blood pressure during the day is higher than normal. Daily ECG monitoring (from August 16, 2016): bradycardia during the observation period, pronounced during the day. Circadian index 136%. During the observation period, submaximal heart rate was not achieved (52% of the maximum possible for a given age). Sinus rhythm, with heart rate from 32 to 101 (average 50) beats.min throughout the observation. Ventricular extrasystole grade 1 according to Ryan. Pathological supraventricular arrhythmias, uncharacteristic of healthy individuals, are recorded. Ventricular ectopic activity is within normal limits. No ischemic ECG changes were detected. No significant changes in the QT interval were detected during the observation period. Is it necessary to do coronary angiography now? It’s kind of scary, they say that this manipulation is not entirely harmless. Please advise what to do? Thank you !
The question is closed
IBS
coronary angiography
angina pectoris
No reward
For whom is CT of the heart vessels contraindicated?
- pregnant women at any stage (the study creates radiation exposure to the fetus, which can affect its development);
- chronic kidney failure (due to impaired renal function, it is difficult to remove radiopaque contrast from the patient’s body, which is fraught with intoxication and allergic manifestations);
- lactation period (the contrast will end up in breast milk through the bloodstream, which is undesirable for the baby; you can breastfeed the baby two days after;
- allergic reaction to iodine - the main component of enhancement drugs;
- severe conditions (patients with severe injuries or depressed consciousness are not subject to tomography, as it may worsen their condition);
- patients with body weight above 200 kg.
Risks of coronary angiography for the patient
Since diagnosing coronary blood flow involves puncturing a peripheral artery of the thigh or shoulder, inserting a catheter through it, moving it through the aorta and coronary vessels, and supplying a contrast iodine-containing substance, this may be accompanied by a negative reaction of the body.
The risk of complications increases if the patient suffers from:
- arterial hypertension;
- diabetes mellitus;
- widespread atherosclerosis;
- acute coronary insufficiency;
- tendency to allergic reactions;
- kidney pathology;
- weakness of the contractile function of the heart;
- rhythm disturbance;
- obesity or underweight;
- chronic alcoholism;
- systemic vasculitis;
- infectious disease.
Depending on the stage of coronary angiography, it can cause the following complications:
- puncture of a peripheral artery - bleeding, hematoma, false aneurysm, fistula between artery and vein, wall dissection, thrombosis, embolism, vascular spasm, infection, allergy to painkillers;
- contrast – allergy, anaphylaxis, intoxication, kidney damage;
- administration of heparin - a decrease in blood clotting ability and, as a result, bleeding;
- insertion of a catheter - arrhythmia, embolism with parts of a cholesterol plaque, dissection of the aorta or coronary vessels, heart attack, stroke.
We recommend reading about coronary angiography of the heart vessels. You will learn about indications and contraindications for the procedure, preparation and performance of coronary angiography, recommendations during the recovery period. And here is more information about bypass surgery of the heart vessels.
Methods for checking cardiac vessels, alternative to CT

Based on them, indirect conclusions are made about the presence of atherosclerotic plaques on the walls of the arteries. Among them is electrocardiography (ECG). Reflects signs of myocardial ischemia. In the asymptomatic form of IHD, tests are carried out with physical exercises that provoke the disease. It is possible to assume a violation of the patency of vascular beds, but it is impossible to determine the local location of areas of their narrowing.
Alternative methods include echocardiography. The diagnostic procedure will show the thickness of the walls of the heart muscle, its chambers, the level of blood pressure in them, the condition of the valves, and the speed of blood flow. However, it will not replace tomography. Its analogue is CT angiography of the heart vessels.
Incidence of complications, risk factors
Like any invasive intervention, coronary angiography can have complications. Their severity ranges from minor and short-lived complications to life-threatening situations that can lead to irreversible consequences. Fortunately, thanks to improvements in equipment and increased experience of medical personnel, the incidence of complications has decreased significantly.
The risk of complications increases with the patient's advanced age, renal failure, uncontrolled diabetes mellitus, and obesity. From the cardiovascular system, the risk is influenced by the severity of coronary heart disease, features of the anatomy of the coronary arteries, the clinical situation (acute myocardial infarction, cardiogenic shock), congestive heart failure, low contractility, recent stroke or myocardial infarction, tendency to bleeding. The incidence of complications is also influenced by the experience of the medical personnel who perform coronary angiography.
However, severe complications are quite rare, occurring in less than 2% of patients; mortality rates are less than 0.08%.
What is coronary angiography and what is it also called?
Coronary angiography is an x-ray of the heart vessels into which a contrast agent has been previously injected. Thanks to this, the lumen and inner walls of the arteries are clearly visible. This allows timely diagnosis of blood clots, tissue tears, etc. To create contrast, the substance urografin is used.
The procedure received this name because coronary means the vessels that bring blood to the myocardium, and graphy is the generalized meaning of all x-ray studies.
You can also find the following designations:
- coronary angiography;
- coronary angiography;
- angiogram.
MRI of open cardiac vessels
An examination method such as MRI is a highly accurate procedure, but at the same time, it is sometimes quite uncomfortable for the patient. Firstly, the patient needs to remain in a lying position for a long time, remaining motionless. Secondly, the tomograph makes loud tapping sounds during operation. This inconvenience can be reduced by using earplugs.
Third, the MRI machine is designed like a tube or tunnel, so patients who are nervous about being in a confined space can ask the medical staff to inject a sedative to make the procedure more comfortable. However, this disadvantage applies only to closed-type MRI, or closed-loop MRI. There are open type tomographs. Open-circuit MRI is ideal for patients who cannot tolerate closed-circuit environments, as well as those whose weight, waist, and chest circumference do not allow for closed-circuit examinations.
In general, we can say that any inconvenience associated with MR coronary angiography is surmountable and not critical. It is quite possible to put up with them in order to obtain accurate diagnostic results.
Recommendations after the procedure
To minimize the risk of complications, the doctor after coronary angiography gives detailed instructions on how to behave in the postoperative period:
- You can stay in the clinic for up to 24 hours;
- Immediately report any unpleasant sensations to a doctor - a safety issue;
- drink plenty of fluids to prevent thrombosis due to dehydration and stress;
- do not engage in sports or any physical activity for a couple of days, avoid hypothermia or overheating;
- Forget about alcohol for three days.
Within two weeks from the date of the CG, you should visit a doctor to assess the patient’s general condition.
Complications
Possible complications of coronary angiography include:
- massive bleeding as a result of physician error (iatrogenic complications), sometimes with fatal outcome;
- angina attack;
- AMI;
- ONMK;
- rupture of a vessel or chambers of the heart;
- allergy to contrast (without prior allergy testing);
- thrombosis;
- arrhythmias;
- thrombocytopenia while taking Heparin;
- secondary infection due to violation of the rules of asepsis and antiseptics;
- respiratory failure;
- kidney damage;
- pressure drop to the point of collapse;
- arterial dissection;
- hematomas at the access site;
- local vascular damage.
To eliminate the negative consequences of CG, it is important to choose a qualified specialist and follow postoperative management of the patient in accordance with the severity of the condition.
Indications for use
The coronary angiography procedure is indicated for: pain in the chest area of unknown origin, retrosternal discomfort that interferes with the patient’s quality of life, in preparation for cardiac surgery and after it to assess the effectiveness. Coronary angiography is prescribed for shortness of breath of unknown etiology, to determine the lack of results from the therapy for cardiovascular diseases, for suspected heart failure, chest injury, suspected atherosclerosis with narrowing of the lumen of the arteries.