Classification
There are several types of crystals:
- Oxalates
are salts of calcium oxalate. - Urates
are salts of uric acid. - Phosphates
are salts of phosphoric acid: amorphous phosphates, tripel phosphates, calcium phosphate, magnesium phosphate. - Carbonates
are calcium salts of carbonic acid. - Bilirubin crystals.
- Cholesterol crystals.
- Crystals of amino acids:
tyrosine, leucine. - Crystals of medicines:
antibiotics, antiviral drugs, etc.
Causes of crystalluria
Almost all types of urinary crystals can be detected in small quantities in a random urine sample from any healthy person. One should suspect any disease or pathological condition only if they are constantly present and in large quantities. The exception is crystals of cholesterol, amino acids and bilirubin, the detection of which always indicates the presence of pathology.
Oxalate crystalluria
The most common salts found in urine are oxalates. Normally, about 30 mg of oxalates are excreted in the urine per day in a dissolved state. They begin to crystallize when urine is left at room temperature for a long time. They have the shape of colorless octahedra, in appearance reminiscent of postal envelopes or pyramids. Oval-shaped oxalates, like hourglasses and gymnastic weights, are also found.
Sometimes it is difficult to differentiate ovoid oxalates and red blood cells based on morphology. To do this, add a drop of acetic acid to the urine sediment, which causes lysis of red blood cells. With parenchymal or obstructive jaundice, ovoid oxalates are stained yellow or dark yellow with bilirubin, while oxalates in the form of octahedrons remain colorless. Spherical oxalates, similar to fat droplets, are found in patients with chronic glomerulonephritis.
There are primary and secondary crystalluria. Primary oxalaturia (oxalosis) is a genetically determined metabolic disorder in which there is deposition of oxalates in the internal organs, their excretion in the urine increases, which contributes to the rapid development of calcium oxalate urolithiasis.
Secondary oxalaturia can have many causes:
- Eating foods high in oxalic acid (spinach, sorrel, potatoes) and ascorbic acid (citrus fruits, rose hips).
- Taking excess vitamin C.
- Vitamin B6 deficiency.
- Diseases accompanied by malabsorption syndrome - celiac disease, Crohn's disease, chronic pancreatitis.
- Dehydration.
- Previous operations on the intestines.
- Ethylene glycol poisoning.
- Oxalate urolithiasis.

Crystalluria
Urate crystalluria
In second place in terms of frequency of occurrence is urate crystalluria. When present in large quantities, uric acid crystals turn urine brick-red. Most often, urates are diamond-shaped, yellow or brownish in color, and sometimes colorless. When taking acetylsalicylic acid, they may turn gray-violet or black. In some cases, urates have pronounced polymorphism - they can be presented in the form of a barrel, a grindstone, or a spindle.
Sometimes they resemble crystals of cholesterol, cystine, or red blood cells, which makes it difficult to identify them. The ability of urates to dissolve in sodium and potassium hydroxide, as well as information about the urine environment (must be acidic), helps in differential diagnosis. This type of crystalluria can be found in a healthy person whose diet consists mainly of meat foods.
Prolonged uraturia indicates a high concentration of uric acid in the blood (hyperuricemia) due to its increased formation. Uraturia can be observed in the following pathologies:
- Gout.
- Dehydration.
- Hemolytic anemia.
- Polycythemia.
- Tumor lysis syndrome when taking chemotherapy drugs (especially in patients with myelo- and lymphoproliferative diseases).
- Wilson-Konovalov disease.
- Diabetes mellitus type 2.
- Urate urolithiasis.
Phosphate crystalluria
There are 4 main types of crystals of phosphoric acid salts - amorphous phosphates, neutral magnesium phosphate, neutral calcium phosphate, tripel phosphates. The most common cause of phosphaturia is the consumption of dairy products, as well as large amounts of plant foods, which contribute to a shift in urine pH to the alkaline side. Other etiological factors:
- Urinary tract infection (tripelphosphates).
- Primary hyperparathyroidism.
- Vitamin D deficiency.
- Pathologies of the kidney tubules - renal tubular acidosis, aminoaciduria, phosphate diabetes.
- Rheumatoid arthritis.
- Iron-deficiency anemia.
- Phosphate urolithiasis.
Amorphous phosphates
The synonymous name is phosphate soils. Under a microscope, they look like colorless amorphous masses, consisting of small balls and grains, grouped into piles of different sizes. Their presence in the urine often causes it to become turbid, and after centrifugation, a white precipitate resembling leukocytes forms at the bottom of the tube.
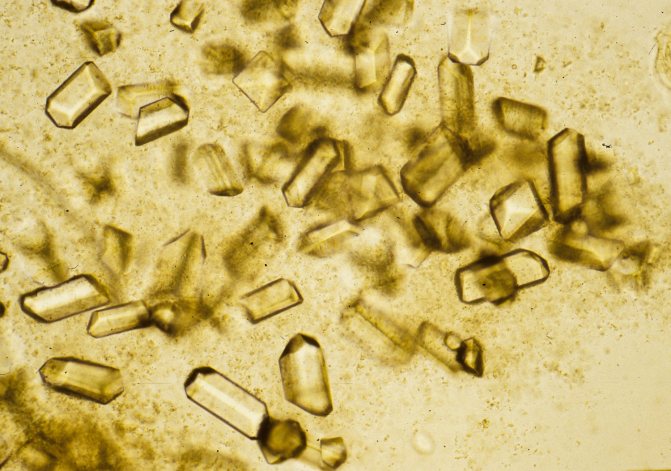
Tripelphosphates
Synonym: ammonia-magnesium phosphate. They are transparent, colorless crystals that resemble coffin lids. If the patient has a pathology of the liver or biliary tract, with prolonged standing of urine, tripel phosphates turn yellow with bilirubin.
Magnesium phosphate
Synonym: neutral magnesium phosphate. Crystals can have different shapes - oblong tablets with strong light refraction, trapezoid, flat plate.
Calcium phosphate
Another name is neutral phosphate of lime. The crystals are colorless prisms with pointed ends. They can be located isolated or grouped, forming rosettes. Sometimes they look like plates or bundles of needles resembling tyrosine.
Carbonaturia
Calcium carbonate in urine is rare. Salts have the form of small balls, molded together, folded into the shapes of drumsticks or gymnastic weights. Often combined with tripelphosphates and amorphous phosphates. They are better visualized after urine has been kept in room conditions for a long time. Calcium carbonate can be seen in the urine of a person who eats a lot of plant foods.
Hippuraturia
A healthy person excretes small amounts of hippuric acid in the urine. An increase in its concentration with subsequent crystallization can occur with the consumption of fruits and berries (lingonberries, plums, pears), benzoic and salicylic acids. Hippuraturia is also characteristic of putrefactive colitis, liver diseases, and gall bladder. Hippuric acid has the form of colorless rhombic tablets with beveled ends.
Bilirubin crystals
Bilirubin is a bile pigment and is excreted in urine in minimal quantities. As the concentration of direct bilirubin in the urine increases, it crystallizes. This is observed when liver cells are damaged (alcoholic or viral hepatitis, cirrhosis) or when bile outflow is impaired (cholecystitis, cholelithiasis, primary sclerosing cholangitis).
Bilirubin crystals can also be detected in diseases accompanied by proteinuria (glomerulonephritis, nephropathy due to autoimmune pathologies or hematological malignancies). This is explained by the fact that when the glomerular apparatus of the kidney is damaged, indirect bilirubin is able to enter the urine, which is not normally observed. Microscopically, bilirubin is presented in the form of yellowish-brown granules or needles collected in bunches. They are often superimposed on leukocytes, cells of flat, transitional epithelium.
Cholesterol crystals
When cholesterol crystallizes in urine, it takes the form of very thin diamond-shaped tablets overlapping each other. Often, along with them, it is possible to identify drops of fat, renal epithelial cells in a state of fatty degeneration, and hyaline casts with fat deposits. Reasons for detecting cholesterol in urine:
- Glomerulonephritis with minimal changes (lipoid nephrosis).
- Nephrotic syndrome.
- Echinococcosis of the kidney.
- Amyloidosis.
Amino acid crystals
Cystine
Cystine crystals are hexagonal thin plates of regular or irregular shape. For the purpose of differential diagnosis, a test for cystine is used - 5% sodium cyanide and 5% sodium nitroprusside are added to the urine. Purple-red coloration indicates the presence of cystine. There are 2 clinical forms of hereditary cystine metabolism disorder:
- Cystinosis - characterized by the deposition of cystine in organs and tissues, increased excretion of cystine in the urine and the formation of cystine stones in the kidneys.
- Cystinuria is a more benign form. The release of cystine is increased, the risk of stone formation is increased, cystine deposition in tissues does not occur.
There is also secondary or acquired cystinuria. Its reasons are as follows:
- Viral hepatitis.
- Cirrhosis of the liver.
- Hepatolenticular degeneration.
Leucine and tyrosine
Normally, these amino acids are excreted in urine in small quantities. Their crystallization occurs with increasing concentration. Leucine is represented by matte-shiny balls of various sizes with concentric striations, located separately or in clusters. Tyrosine has the appearance of thin, small needles grouped into bunches or asterisks.
Crystalluria of these amino acids is observed with genetic metabolic disorders or extensive tissue and cellular decay:
- Tyrosinemia.
- Leucinosis (maple syrup disease).
- B-12 deficiency anemia.
- Leukemia.
- Malignant neoplasms.
- Myasthenia.
- Phosphorus poisoning.
Drug-induced crystalluria
Detection of drug crystals in urine often occurs with long-term use or overdose. The formation of drug crystals can block the kidney tubules and cause acute kidney injury. Basically, drug crystals have the form of thin needles or small rectangles. Most often, drug-induced crystalluria develops while taking:
- Antibiotics – ampicillin, amoxicillin.
- Antiviral agents - acyclovir, indinavir.
- Sulfonamides – sulfamethoxazole.
- Vitamin C.
- Barbiturates – phenobarbital.
- Antitumor drugs – methotrexate.
- Potassium-sparing diuretics – triamterene.
Urates under a microscope
How do phosphates form?
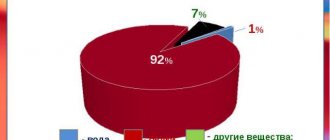
Phosphates are chemical compounds that are formed during the reactions of alkaline solutions and phosphoric acid. These substances enter the body with food and liquid.
Phosphorus itself is a fairly valuable element; up to 85% of all phosphates are found in teeth and bone tissue. The rest are located in the brain matter, cell DNA and muscles. In order to function properly in the body, phosphorus must be bound to calcium, this ensures proper muscle contraction and fermentation of important substances.
Phosphorus should be present with calcium in the body in a ratio of one to two, which is half the calcium saturation level. An increase in phosphates leads to intense leaching of calcium, which softens bones and destroys teeth. Vitamin D plays a major role in the metabolism of calcium and phosphorus.
To maintain the phosphorus-calcium balance, the body flushes out the excess during human urination. In some cases, tripelphosphate salts are found in the urine due to an increase in the alkaline balance of urine (pH>7) and deposition of ammonia, phosphate salts and magnesium.
More on the topic: What causes increased ketone bodies in a child’s urine?
Diagnostics
Despite the fact that crystals are quite common in normal urine, repeated detection of crystalluria requires a visit to a general practitioner to determine the cause. When interviewing the patient, the nature of the person’s diet is clarified, what medications he is taking, and whether he is registered with a dispensary. An additional examination is prescribed, including:
- General blood analysis.
The level of red blood cells and hemoglobin is examined, which can be either decreased or increased. - Blood chemistry.
In case of impaired renal excretory function, the concentration of urea and creatinine is increased; in diseases of the hepatobiliary system - ALT, AST, direct bilirubin. With gout, there is an increase in uric acid levels in the blood. Biochemical markers of hemolysis are LDH, indirect bilirubin. People with Wilson-Konovalov disease have decreased levels of ceruloplasmin and increased amounts of copper in the blood. - Analysis of urine.
Indicators of a general urinalysis (leukocyturia, hematuria, proteinuria) and other findings during microscopy of urine sediment (epithelial cells, formed elements, casts) can help in identifying the cause of crystalluria. Biochemical analysis of 24-hour urine for oxalates and calcium is the gold standard for diagnosing oxalosis. - Amino Acid Metabolism Study
. If amino acid crystals are detected, the concentration of tyrosine, leucine, cystine in blood serum and urine is measured. - Instrumental research.
If there is a suspicion of urolithiasis, a kidney ultrasound is prescribed, which can visualize stones, as well as excretory urography, which allows one to assess the presence and degree of urinary tract obstruction.
Relationship between phosphaturia and diet
Phosphates appear in urine most often when the body is alkalized by consumed foods. As a result, phosphaturia can be combated by following a strict diet. To do this, you need to stop taking foods that increase the alkaline reaction in the body.
These include:
| № | Helpful information |
| 1 | soda and alcohol of any strength |
| 2 | fermented milk products, curdled milk, cottage cheese, yogurt |
| 3 | sweets, baked goods |
| 4 | fish and fatty meats, lard, rich broths |
| 5 | animal fats, margarine and butter |
| 6 | crackers and chips with flavors and dyes |
| 7 | salt intake should be reduced to 2 grams per day, including cooking |
Experts recommend including the following products in your diet more often:
- rosehip decoction, herbal teas, chicory, fresh unsweetened juices;
- various cereals and porridges made from them;
- all types of legumes, lentils, peas and beans;
- a large number of vegetables, pumpkin, carrots, peppers, zucchini and cucumbers;
- fish and lean meat;
- a handful of any nuts;
- increase consumption of grapes, figs, apples and plums;
- Use eggs and all types of cheese with caution.
More on the topic: Types of bladder exstrophy and treatment methods
Correction
Conservative therapy
In the vast majority of cases, dietary recommendations are sufficient for the disappearance of crystalluria - drinking plenty of fluids, a balanced diet of plant and animal foods. Patients with hereditary hyperoxaluria are prohibited from taking foods rich in oxalic and ascorbic acids. People with amino acid metabolism disorders are prescribed a strict diet with the maximum possible limitation of tyrosine, leucine, and tryptophan.
In case of drug crystalluria, discontinuation of the drug or reduction of its dosage is required. Conservative therapy for crystalluria directly depends on the cause:
- Vitamins, microelements.
Vitamin B6 and magnesium can suppress the crystallization of oxalates, so they are prescribed for oxalosis. To prevent phosphaturia caused by secondary hyperparathyroidism, vitamin D preparations (cholecalciferol) are used. - Antibacterial agents.
For urinary tract infections, fosfomycin trometamol, penicillin antibiotics (amoxicillin) and cephalosporins (cephexime) are used. - Allopurinol.
This drug suppresses the formation of uric acid. It is prescribed for gout and patients undergoing chemotherapy to prevent acute urate nephropathy, a typical complication of tumor breakdown syndrome. - Preparations for alkalinizing urine.
Sodium citrate or sodium bicarbonate are used to treat many tubulopathies accompanied by tubular acidosis and genetic disorders of amino acid metabolism, as well as to dissolve urate and oxalate stones. - Cysteamine.
This drug reduces the intracellular content of cystine, so its use is indicated for patients with cystinosis and primary cystinuria. - Litokinetics.
For small stones, the use of alpha-blockers (tamsulosin) and calcium channel blockers (nifedipine), which relax the smooth muscles of the ureters, which promotes the spontaneous passage of stones, is justified.
Surgery
For patients with urolithiasis, depending on the size of the stones, their shape, location, various methods of removal are indicated - shock wave lithotripsy (destruction by directed ultrasound), laparoscopic or open surgery. For cholelithiasis, laparoscopic cholecystectomy is performed.