What is proper breastfeeding and why is it so important?
- What can signal us that the baby is not latching onto the breast correctly when sucking?
- Why is it necessary to learn how to properly attach a baby to the breast?
- What could be the reasons that a child has stopped latching on to the breast correctly?
- Basic principles of teaching your baby to latch on to the breast correctly
- How to teach a baby to open his mouth wide for breastfeeding?
- Ways to help your baby latch on correctly
Basic principles to teach your baby to properly latch on to the breast during feeding:
Your nipple should be deep enough in your baby's mouth! When the breast is latched correctly, the baby sucks not on the nipple, but on the areola. For example: Run your tongue across the roof of your mouth. Closer to the throat is the soft palate, this is where your nipple should be located on the baby.
Otherwise, during feeding, the skin of the nipple is injured and cracks may appear. And the baby receives little milk and does not eat enough.
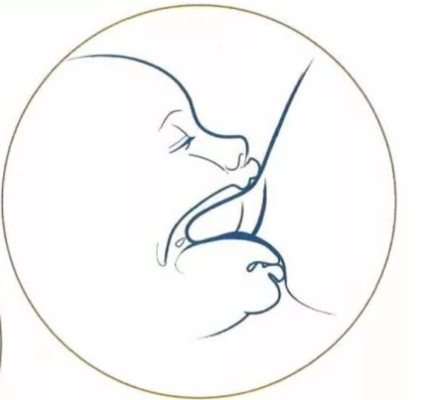
Notice how deep the nipple is located in the baby's mouth (picture on the right). Thus, breast milk goes directly into the throat, bypassing the surface of the tongue. As you know, during the sucking process, the child’s tongue creates wave-like sucking movements. They are the source of nipple injuries if applied incorrectly.
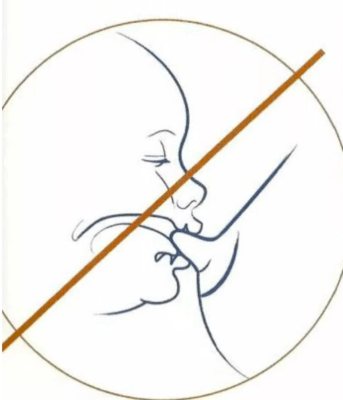
The second picture shows that the nipple of the mother's breast is located directly on the baby's tongue.
When a baby sucks on a pacifier, he makes the same movements as when he attaches incorrectly. No nipple will be completely comparable to a woman's breast during feeding. Which forces the baby to open his mouth wide and make sufficient efforts to obtain breast milk.
Feeding a baby with a bottle teaches him to open his mouth a little and not to strain too much (the milk almost flows by itself). Yes, drinking from a bottle is much easier than from the breast! Therefore, it may happen that the baby begins to latch onto the breast incorrectly, becomes capricious at the breast, and you may experience soreness and cracked nipples.
How do you know if your baby is latching deep enough?
There are several signs.
- Asymmetry
. What this is is very easy to understand if you let your child suck your finger. Stroke the baby's tongue - he will begin to suck. And if you turn your finger over and make a “come to me” movement with its pad across the palate, the child begins to suck much harder. Those. correct grip is when
nipple touches soft palate (in the mouth above the tongue, the first part of the palate is called the hard palate, and the second, deeper inside, is called the soft palate). This triggers a powerful sucking reflex. As doctors say, “the child will suck on anything, you just need to give it to him correctly!” To do this, the application must be asymmetrical, i.e. The breast looks with the nipple not into the child’s mouth, but upward, into the palate. Then a much larger piece of the breast will be captured below than on top. For this purpose, it is optimal to feed not in the usual Madonna position, but from under the arm or in the so-called. “cross cradle”, when the baby is held with the opposite hand (left hand at the right breast, for example). When attaching, the baby’s neck is supported by the mother’s palm and, by moving her hand, the mother helps maintain a deep grip (see more about poses).
- Tongue ON gum
. Try squeezing your teeth - you can squeeze very hard.
Now put it on your teeth tongue and try to compress. Much less power! When the child sucks properly, he places his tongue on the gum and squeezes not too hard. Mom has no pain! When sucking, the baby presses the tongue on the breast, making wave-like movements and squeezing milk into the mouth, and then sucking it in using a vacuum. The tongue should move freely and stick out far enough. When sucking incorrectly, the tongue remains inside the mouth and the gums shrink much more painfully; milk flows worse. It is necessary to ensure that the child's tongue sticks out. If a child is used to sticking out his tongue shallowly, he can be taught to stick it out further with the help of deep attachment, a favorable feeding position and special exercises (see smoothing the tongue). But it happens that the baby is physically unable to stick out his tongue due to a short frenulum. In this case, you will need to trim it. What is a short frenulum?
A short frenulum of the tongue is one of the common problems when feeding,
in this case, the tongue simply cannot stick out forward to the teeth and the latch is shallow, often painful, or there is no pain, but the child cannot suck out enough milk and remains hungry (at the same time, he may cry a lot, often asks for the breast, and sits on it for a long time “ hanging"). Try to lightly touch the lower lip of an awake child - he will most likely open his mouth wide and stick out his tongue, the tongue should stick out forward onto the gum and beyond. In the pictures on the right there is a pronounced short frenulum (the membrane connecting the tongue and the lower part of the oral cavity). A characteristic sign is that when the tongue protrudes, the tip has the shape of a heart (however, this is not necessary; there are different types of short frenulum). Here are more pictures
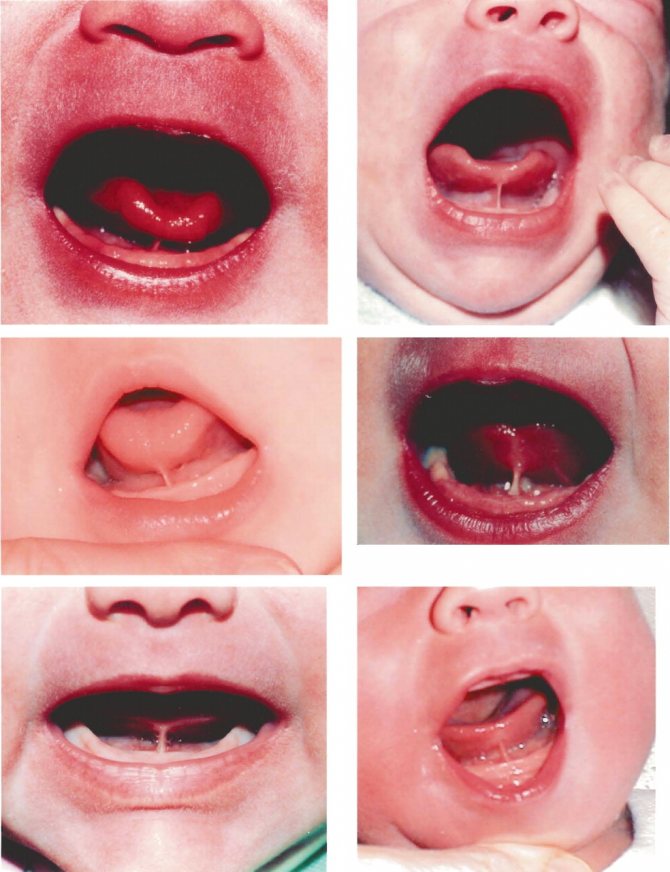
. A detailed article about the short frenulum from the site am-am.info Short frenulum in newborns and breastfeeding. More materials about the short frenulum - a selection from our website “Short frenulum of the tongue and lips.” - Wide open mouth
.
Another common gripping problem is that the mouth is not open wide enough. With a deep grip, the child’s lips are separated as much as possible, the angle is 130-150 degrees or even wider . When the latch is ineffective, the mouth is opened 90 degrees or less. In this case, in the place where the baby's lower jaw presses, there may be pain during feeding (although this is not necessary).
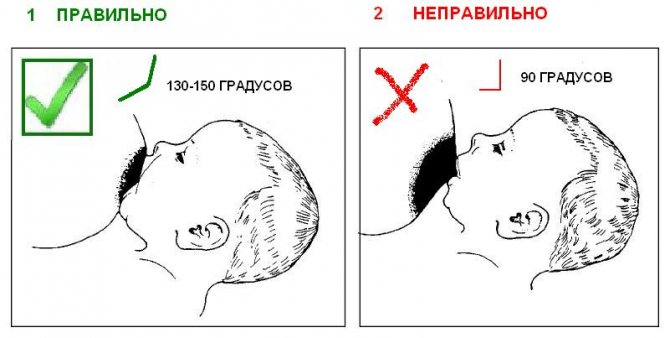
If it hurts to feed, your baby may not have opened his mouth wide enough . Why did this happen? Perhaps in this position it is simply uncomfortable for the child to open his mouth wide. Take an imaginary thick, thick hamburger in your hand, raise it to the level of your mouth, and try to bite it. Mouth opened wide? Now raise the imaginary hamburger to the level of your nose and try to bite again. The mouth opens itself much wider!
To open your mouth wider, it often helps to adjust your posture, more on that below.
Video: you can clearly see that milk flows much worse if not enough of the areola is captured (video by Jack Newman).
——————————-additional information———————————————- 4. Sucking mechanism
.
When sucking, the baby makes several movements at the same time. The lower jaw moves up and down, while the uvula makes a wave-like movement from the tip to the base of the tongue, squeezing milk from the expansion of the ducts under the areola and then sucking it in using a vacuum. As you can see, the mechanism is strikingly different from bottle sucking , in which it is enough to open your mouth slightly and lightly press up and down on the nipple. That is why in the first weeks of feeding it is not recommended to give the baby a bottle and a pacifier, so that he does not start sucking at the breast like a bottle (which means it is painful for the mother and/or not getting enough milk). 5. Other signs
.
At the beginning of sucking, the baby makes short, quick movements until milk begins to come out of the breast (the “flux” begins). Then the rhythm changes and the baby switches to more constant deep sucking, with pauses. There is one sip per sucking, no more . Pauses mean that the milk is flowing well. Ideally, at the beginning of feeding there is always a phase of deeper and slower sucking “on the tide”. The baby's cheeks are rounded, not retracted.
Sometimes the ears move when sucking. After sucking, the nipple comes out elongated and round, symmetrical, and not flattened or slanted. Another possible problem in which the latch remains painful, even if it looks correct, is a high palate in a child. A little information.
Videos: The first few videos on the list perfectly illustrate where the latch is good and the baby is sipping and where it is not (Jack Newman website).
How to teach a baby to open his mouth wide for breastfeeding?
To effectively latch onto a larger area of the breast (both nipple and areola), the baby needs to open his mouth wide.
If a child does not know how (newborn) or has forgotten how (confusion due to bottles and pacifiers), he can be taught.
- – When communicating with a baby, show him how you open your mouth wide. It sounds funny, especially in the case of a newborn, but don’t think, just do it. Baby mammals tend to instinctively try to repeat everything that their mother shows. In most cases, when looking at you, he will open his mouth imitatively.
- – Another option: holding the baby at the breast, run your nipple over the baby’s face, in the area of the nasolabial triangle. On the chin, nose, cheeks. You will see how the baby opens his mouth and moves towards the nipple, trying to grab it.
When to start feeding your newborn
Surely, you have more than once watched with emotion videos in which newly born baby animals, hobbling on legs trembling from weakness or funny moving their paws, reach for their mother’s nipple. These tiny, often still blind lumps are controlled by a powerful force - the thirst for life. This is how nature ordered it.
And the health of the little man largely depends on how quickly after birth he is put to the breast . The colostrum released in the first hours is a real mother’s blessing for her baby to lead an independent life. This is a powerful amulet against many infectious (and other) diseases and an invaluable source of nutrients.
Unfortunately, colostrum very quickly loses its beneficial properties, remaining just a high-calorie food after just a few hours. Therefore, for many years, the World Health Organization has strongly recommended that all babies be put to the breast immediately after birth. Not for feeding - for a healthy future .
Not all children, being in a state of postpartum stress, are able to immediately actively suck. Don't worry: the first tiny drops of colostrum are easily released when you press on the areola. The baby will just have to lick them off. Then he will sleep soundly for several hours, resting after a difficult period of childbirth. But when should a mother start to really feed him, teaching him to latch on correctly - read here.
Ways to help your baby latch on correctly.
The first method is called BIOLOGICAL NATURE.
The mother undresses to the waist and the child must be undressed (the diaper can be left on). You need to sit on a bed or chair at an angle of 45 degrees. For comfort, you can place pillows under your back and legs. There should be no discomfort - make yourself as comfortable as possible! Remember: a relaxed mom = more oxytocin release = better milk flow from the breast.

The baby is placed vertically between the breasts. At the same time, both mother and child should be warm. If necessary, cover yourself with a blanket. And then the child does everything himself; you can only guide and help him a little. Lying between the breasts, he reaches one of the nipples, opens his mouth wide and begins to suck on the breast. Then you simply put the child on your arm (you can also put a pillow under your arm so as not to strain)
This is an amazing way of attaching, but it is the one that triggers the baby’s search reflex, which even premature babies have.
By the way, the position on the stomach is magical for a child. He feels safe, feels the warmth and closeness of his mother, her heartbeat. And the most amazing thing is that he smells the amniotic fluid (the water of the amniotic sac), which is released from the Mangomery glands - small pimples near the nipples!
How to properly attach a baby to the breast
With the correct latching technique, feeding does not cause any difficulties for either the mother or the baby. Please note: the baby will latch onto the nipple correctly if he not only has his mouth open, but also his tongue is stuck out a little forward and curved in a boat shape . Then he will accept mother’s breasts tenderly, as if in folded palms, and he will suck on them so that the movements of his rough tongue will give mother unearthly pleasure.
The technique of proper breastfeeding is described in detail here. Compliance with it will 99% protect a woman from the formation of monstrously painful nipple cracks, from lactostasis and mastitis. And the baby will not suffer from intestinal colic and endless regurgitation.
How to feed a baby without pain? Cracks and abrasions on the chest.
10.09.2016
.

One of the first problems that young mothers often face in the maternity hospital are cracks and abrasions on the nipples. Causing intense, sometimes unbearable pain, they greatly complicate the already difficult postpartum period. At such moments, in the absence of special knowledge and support, a woman is often faced with a choice - to endure and give the baby the breast, overcoming the pain, or to stop putting the baby to the breast and switch to feeding with expressed milk, or even to artificial feeding!
Often, even in specialized medical institutions, mothers are advised to limit the time the baby stays at the breast, feed the baby strictly according to the schedule, purchase and use breast pads during feeding, and use wound-healing ointments. It must be said that at some initial stage, it may indeed seem that these measures help. Short-term relief comes to mom. But it is too short-lived and subsequently only worsens the situation. Why is this happening ? Because neither restriction of feeding, nor pads, nor ointments remove the cause of cracks and abrasions on the nipples.
Causes of cracks and abrasions on the nipples:
- improper attachment of the baby to the breast;
- improper weaning of a child from the breast - in no case should you “pull” the breast out of the child’s mouth. You need to carefully insert your little finger into the corner of the baby’s mouth and only after the baby opens his mouth, take the breast.
- short frenulum of the tongue in a child. If you suspect a short frenulum of the tongue, it is necessary to show the child to a pediatrician or dentist.
- frequent breast washing and additional treatment of the breast skin with antiseptics.
The main reason for the occurrence of cracks in the nipples is not the fact of the child sucking the breast and its duration, but an incorrect grasp of the breast, and therefore incorrect sucking.
With such improper sucking, the child grasps only the nipple itself, and the areola is located outside the child’s mouth. The delicate and sensitive skin of the nipple is rubbed by the gums. Mom experiences extremely unpleasant and painful sensations, which only intensify with each feeding.
When a baby suckles CORRECTLY, his gums do not touch the nipple, but are located on the areola. In this case, the nipple ends up deep in the child’s mouth and is not injured, even with prolonged, almost continuous sucking. When properly applied, the baby empties the breast effectively and painlessly, stimulating further milk production. It must be said that improper attachment over time can cause much more serious problems with lactation.
The consequences of improper application, in addition to abrasions and cracks, can be:
- poor breast emptying
- low weight gain in a child
- lactostases
- decreased breast milk production
It should be noted that damaged breast skin is an entry point for infection and threatens inflammation of the glandular tissue of the mammary gland - mastitis.
Unfortunately, the use of breast pads on damaged breast skin and restriction of feedings further contribute to the development of complications. So, through the pad, and even with incorrect attachment, the baby cannot suck out a sufficient amount of milk himself or effectively stimulate the breast for further milk production. As a result, the mother’s milk production decreases, and she is forced to supplement her baby with formula.
What to do?
The only way out is to learn how to properly attach your baby to the breast. As soon as the breasts stop being injured during sucking, the cracks begin to heal. In some cases, local application of antiseptics is required.
Is it possible to prevent the appearance of abrasions and cracks on the nipples or a few words about prevention.
To this day, in some places you can still hear recommendations to rub your nipples with a rough terry towel during pregnancy or to pull them off for several minutes. Supposedly this should make the skin on the nipples rougher and more insensitive. But if you think about it, is this necessary? Since the nipple is injured as a result of improper attachment, and not at all because the skin on the chest is tender and sensitive, there is no point in “hardening” the nipples. Moreover, it can be dangerous. Intensive rubbing of the breast skin with a hard towel can lead to abrasions and microcracks, through which infection can penetrate into the mammary glands. Additionally, nipple stimulation during pregnancy can lead to premature and unwanted uterine contractions.
Instead, it is better to study as much RELIABLE and up-to-date information about breastfeeding as possible during pregnancy. Perhaps the best solution would be to attend a meeting of nursing mothers and see with your own eyes how to properly attach a baby to the breast, in what positions you can and should breastfeed, and how to safely remove the breast from a baby. There you can ask all your questions to both women who are successfully breastfeeding and the lactation consultants . Let early education be the first step to long-term and successful feeding of your baby with MOM'S MILK!
Author of the article, lactation consultant, obstetrician-gynecologist, Galina Fomicheva
Urgent call to a breastfeeding specialist: 99-08-34 more details
Calling a breastfeeding consultant Feeding clothes, slings
Did you like the article? 39
Share











